Stroke Rehabilitation
Stroke Rehabilitation
Course Description
Strokes are a leading cause of death in the U.S. and the leading cause of disability (“Prevention”). No one plans to have a stroke and when it occurs it is shocking and scary to the stroke victim as well as the family. Emotions such fear, depression, anger, and sadness will immediately creep in and rightfully so. And that’s why rehabilitation is so important. Read more to discover in depth infromation about CVA, the nurse's role in rehabilitation, and strategies.
Accreditation Information: KLA Education Services LLC is accredited by the State of California Board of Registered Nursing, Provider # CEP16145.
Course Certification: Once you have completed this course, click on the “Print Certificate” option below to save or print your CE course certification. If you are not yet registered in a course plan with IvyLeagueNurse, please complete the registration and payment process so that you are able to log into your account and fully obtain your course certificate. Our affordable and unlimited one-year CEU plan starts at just $19.99.
Print Certificate Print Course
Course Objectives
Upon completion of this course, the course participant will be able to:
- Define stroke or CVA.
- Discuss the nursing role in stroke rehabilitation.
- Discuss four common principles and strategies used in stoke rehabilitation.
- Identify five strategies in the rehabilitation of stroke patients with self-care deficits and mobility issues.
- Describe five techniques in the rehabilitation of stroke patients with communication and swallow difficulties.
- Discuss stroke prevention and education.
Course Content
What is a Stroke?
A stroke, sometimes called a "brain attack," occurs when blood flow to an area in the brain is cut off. The brain cells, deprived of the oxygen and glucose needed to survive, die. If a stroke is not caught early, permanent brain damage or death can result.
Types of Stroke
There are two major stroke classifications:
-
Ischemic stroke occurs when a clot in a vessel of the brain blocks blood flow to the brain’s cells causing oxygen deprivation with subsequent tissue damage. The term ischemic refers to an insufficient blood supply. Eighty percent of all strokes are ischemic ("Stroke: Hope Through Research").
-
Hemorrhagic stroke occurs as a bleed within the brain, often causing tissue damage due to pressure-related changes. Most commonly, intracerebral hemorrhages are caused by rupture of vessels due to long-term atherosclerotic damage and arterial hypertension ("Stroke: Hope Through Research").
(CDC, 2010b.)
Transient Ischemic Attack (TIA)
A transient ischemic attack (TIA) is defined as a brief episode of cerebral ischemia that is usually characterized by temporary blurring of vision, slurring of speech, numbness, paralysis, or syncope and is often predictive of a serious stroke “Stroke: Hope Through Research”. It is sometimes called a mini-stroke but resolves in less than 24 hours.
Signs and Symptoms of a Stroke
Knowing the signs and symptoms of a stroke is of vital importance because the time that goes by from the moment of symptoms to the time medical treatment starts can greatly affect the patient’s outcome. For each minute a stroke goes untreated and blood flow to the brain continues to be blocked, a person loses about 1.9 million neurons (“Signs and Symptoms of Stroke”).
Stroke symptoms include:




The Road to Rehabilitation
A patient with stroke like symptoms will be diagnosed shortly after arriving to the ER. Once a patient's stroke has been evaluated and his condition has been stabilized, he'll be transferred out of the ER and into a hospital bed. How long he spends in the hospital depends on a number of factors, including the type and severity of his stroke, what medical complications arise, and the extent of his disability. But it's unlikely that he'll be in the hospital for long. Most people stay in the hospital for 3-6 days after an ischemic stroke and possibly longer after a hemorrhagic stroke.
Stroke Measuring Tool
One of the most important tools healthcare providers use to quantify the severity of a stroke is called the National Institute of Health Stroke Scale (NIHSS). The NIHSS is usually performed during the initial assessment to establish a baseline and then repeated according to the protocol of that particular hospital, which usually includes two hours post treatment such as t-PA, 24 hours after symptoms started, any time the patient is transferred to another floor, and also the day the patient is discharged home or to another facility such as a rehabilitation hospital. Those qualified to perform the NIHSS include physicians, physician assistants, nurse practitioners, and registered nurses ("Frequently Asked Questions from the November 18, 2009, Training Webinar”). The NIHSS is composed of 11 items, each of which scores a specific ability between a 0 and 4. For each item, a score of 0 typically indicates normal function in that specific ability, while a higher score is indicative of some level of impairment ("Stroke Assessment Scales"). The individual scores from each item are summed in order to calculate a patient's total NIHSS score. The maximum possible score is 42, with the minimum score being a 0 ("Stroke Assessment Scales").

The following images and words are used during step 8 and 9:

(http://www.neurologyindia.com)
The stroke scale should be administered in the order listed with the results recorded after each subscale exam. Follow the directions provided for each exam and do not go back and change any answer. Scores should reflect what the patient does, not what the clinician thinks the patient can do. The clinician should record answers while administering the exam and work quickly. Except where indicated, the patient should not be coached ("Stroke Assessment Scales").
Acute Care
The main purposes of acute care are to:
• Make sure the patient's condition is caused by a stroke and not by some other medical problem.
• Determine the type and location of the stroke and how serious it is.
• Prevent or treat complications such as bowel or bladder problems or pressure ulcers (bed sores).
• Prevent another stroke.
• Encourage the patient to move and perform self-care tasks, such as eating and getting out of bed, as early as medically possible. This is the first step in rehabilitation.
Rehabilitation begins in the acute care setting but continues after discharge, sometimes requiring the stroke survivor to work with specialists for months or years. In this particular lesson, we will primarily focus on the nursing care given to stroke survivors that require inpatient rehabilitation after discharge from the acute care hospital.
In the United States more than 700,000 people suffer a stroke each year, and approximately two-thirds of these individuals survive and require rehabilitation (“Post-Stroke Rehabilitation”). The goals of rehabilitation are to help survivors maximize their quality of life and gain as much independence as possible. Rehabilitation does not “cure” a person from the effects of the stroke in that it does not heal the damaged part of the brain, but can greatly improve the survivor’s outcome.
Rehabilitation helps stroke survivors relearn skills that are lost when part of the brain is damaged. For example, these skills can include activities of daily living such as dressing themselves, bathing, and eating breakfast, as well as walking or any other complex physical activity. Rehabilitation also teaches survivors new ways of performing tasks to compensate for any permanent disabilities. For example, individuals may need to learn how to bathe and dress using only one hand, or how to communicate effectively when their ability to use language has been compromised. Most rehabilitation experts agree that for any rehabilitation program to be successful with consistent, positive outcomes it needs to be carefully directed and well-focused with repetitive practice (“Post-Stroke Rehabilitation”).
Nursing Role in Rehabilitation Hospital
Nurses specializing in rehabilitation help patients relearn how to carry out the basic activities of daily living and to do it safely. They also educate the patient and their family/caregivers on how to care for the skin, how to manage transfers between a bed and a wheelchair, and any new medication with their uses and side effects. Rehabilitation nurses also work to reduce risk factors that may lead to a second stroke, and provide training for caregivers. Nurses are closely involved in helping stroke survivors manage personal care issues, such as bathing and controlling incontinence, as well as psychosocial issues as sometimes coping with their new life is often difficult.
But the nursing role would be very ineffective if it weren’t for interdisciplinary team working together to maximize the patient’s outcome. “Better clinical outcomes are achieved when post-acute stroke patients who are candidates for rehabilitation receive coordinated, multidisciplinary evaluation and intervention.
Post-acute stroke care should be delivered in a setting in which rehabilitation care is formally coordinated and organized. Post-acute stroke care should be delivered by a variety of treatment disciplines, experienced in providing post stroke care, to ensure consistency and reduce the risk of complications” (Duncan, "Management of Adult Stroke Rehabilitation Care”).
The interdisciplinary team includes:
-
Physicians
-
Registered Nurses
-
Physical Therapists (PT)
-
Occupational Therapists (OT)
-
Speech and Language Pathologists (SLP)
-
Psychologists
-
Case Manager
-
Nursing Assistants
-
Patient and Family members/Caregivers
A growing body of evidence indicates that patients do better with a well-organized, multidisciplinary approach to post-acute rehabilitation after a stroke (Duncan, "Management of Adult Stroke Rehabilitation Care”).
Stroke Rehabilitation Principles and Strategies for Nurses
Stroke Patients with Self-Care Deficits
Self-care deficit can be defined as an impaired ability to perform or complete activities of daily living, such as feeding, dressing, bathing, toileting.
May be related to:
-
Pain/discomfort
-
Depression
-
Perceptual/cognitive impairment
-
Neuromuscular impairment, decreased strength and endurance, loss of muscle control/coordination


Expected outcomes:
-
Patients can perform self-care activities relative to their capability, safely.
-
Patients can recognize when assistance is needed and identify resources/caregivers to aid in assistance.
Upon admission of the stroke survivor to the rehabilitation unit, the registered nurse will perform the initial head to toe assessment but will collaborate and work closely with the occupational therapists regarding the patient’s self-care deficits as it relates to activities of daily living. Doing this will ensure the patient gets focused, coordinated care that will improve patient outcomes.
Nursing Interventions and Rationale:
-
Assess patient’s capabilities and deficiencies (using a measurable scale) performing daily needs.
-
Rationale: Assist in anticipating / planning needs individually
-
-
Allow the patient to do as much as possible themselves only providing assistance as needed.
-
Rationale: Improves recovery and confidence.
-
-
Monitor impulsiveness related to impaired decision-making.
-
Rationale: May indicate need for intervention and monitoring to enhance patient safety
-
-
Give the patient enough time to complete their task to the best of their ability.
-
Rationale: Improves patient recovery and outcome through repetitive practice.
-
-
Give positive feedback for any work done or success.
-
Rationale: Motivates patient to continue working hard and improving.
-
-
Use personal assistive devices, such as a walker, reacher and grabber, sock assistant, button hook and zipper pull, shoehorn, dressing stick, etc.
-
Rationale: Increases independence and self-esteem.
-
-
Assess patient’s voiding needs and independence. Offer bathroom breaks/assistance when needed.
-
Rationale: Stroke patients often lose control of voiding and may require frequent bathroom breaks to maintain continence and self-esteem.
-
-
Identify the previous defecation habits and return to the normal habits. Recommend appropriate amount of water intake, fibrous foods, and increased activity.
-
Rationale: Prevent constipation and any complications associated with it.
-
Impaired Physical Mobility
Stroke survivors requiring inpatient rehabilitation typically have a degree of impaired physical mobility ranging from mild to severe usually affecting one side of the body. Impaired physical mobility can be defined as a limitation in independent, purposeful physical movement of the body or of one or more extremities.

May be related to:
-
Neuromuscular involvement: weakness, paresthesia; flaccid/hypotonic paralysis (initially); spastic paralysis
-
Perceptual/cognitive impairment
Desired Outcomes:
-
Maintain/increase strength and function of affected or compensatory body part.
-
Maintain optimal position of function as evidenced by absence of contractures, foot drop.
-
Demonstrate techniques/behaviors that enable resumption of activities.
-
Maintain skin integrity.
Physical therapists work together with nursing to achieve the best possible outcome related to impaired mobility. The care is coordinated and reviewed daily by all members of the multidisciplinary team to accommodate the changing needs and goals of the patient and family.
Nursing Interventions with Rationale
-
Assess extent of impairment initially and on a regular basis. Classify according to 0–4 scale.
-
Rationale: Identifies strengths and deficiencies that may provide information regarding recovery. Assists in choice of interventions, because different techniques are used for flaccid and spastic paralysis (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Change positions at least every 2 hr (supine, side lying) and possibly more often if placed on affected side.
-
Rationale: Reduces risk of tissue injury. Affected side has poorer circulation and reduced sensation and is more predisposed to skin breakdown (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Position in prone position once or twice a day if patient can tolerate.
-
Rationale: Helps maintain functional hip extension; however, may increase anxiety, especially about ability to breathe (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Prop extremities in functional position; use footboard during the period of flaccid paralysis. Maintain neutral position of head.
-
Rationale: Prevents contractures and foot drop and facilitates use when function returns. Flaccid paralysis may interfere with ability to support head, whereas spastic paralysis may lead to deviation of head to one side (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Use arm sling when patient is in upright position, as indicated.
-
Rationale: During flaccid paralysis, use of sling may reduce risk of shoulder subluxation and shoulder-hand syndrome (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Evaluate need for positional aids and/or splints during spastic paralysis.
-
Rationale: Flexion contractures occur because flexor muscles are stronger than extensors (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Place pillow under axilla to abduct arm.
-
Rationale: Prevents adduction of shoulder and flexion of elbow.
-
-
Elevate arm and hand
-
Rationale: Promotes venous return and helps prevent edema formation.
-
-
Place hard hand-rolls in the palm with fingers and thumb opposed.
-
Rationale: Hard cones decrease the stimulation of finger flexion, maintaining finger and thumb in a functional position (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Place knee and hop in extended position.
-
Rationale: Maintains functional position.
-
-
Maintain leg in neutral position with a trochanter roll.
-
Rationale: Prevents external hip rotation.
-
-
Discontinue use of footboard, when appropriate.
-
Rationale: Continued use (after change from flaccid to spastic paralysis) can cause excessive pressure on the ball of the foot, enhance spasticity, and actually increase plantar flexion (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
Observe affected side for color, edema, or other signs of compromised circulation.
-
Rationale: Edematous tissue is more easily traumatized and heals more slowly.
-
-
Inspect skin regularly, particularly over bony prominences. Gently massage any reddened areas and provide aids such as sheepskin pads as necessary.
-
Rationale: Pressure points over bony prominences are most at risk for decreased perfusion. Circulatory stimulation and padding help prevent skin breakdown and decubitus development.
-
-
Begin active or passive ROM to all extremities (including splinted) on admission. Encourage exercises such as quadriceps/gluteal exercise, squeezing rubber ball, extension of fingers and legs/feet.
-
Rationale: Minimizes muscle atrophy, promotes circulation, helps prevent contractures. Reduces risk of hypercalciuria and osteoporosis if underlying problem is hemorrhage. Note: Excessive stimulation can predispose to rebleeding (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Assist patient with exercise and perform ROM exercises for both the affected and unaffected sides. Teach and encourage patient to use his unaffected side to exercise his affected side.
-
Rationale: Minimize muscle atrophy and improve mobility and coordination.
-
-
Assist patient to develop sitting balance by raising head of bed, assist to sit on edge of bed, having patient to use the strong arm to support body weight and move using the strong leg. Assist to develop standing balance by putting flat walking shoes, support patient’s lower back with hands while positioning own knees outside patient’s knees, assist in using parallel bars.
-
Rationale: Aids in retraining neuronal pathways, enhancing proprioception and motor response (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Get patient up in chair as soon as vital signs are stable, except following cerebral hemorrhage.
-
Rationale: Helps stabilize BP (by restoring vasomotor tone), promotes maintenance of extremities in a functional position and emptying of bladder, reducing risk of urinary stones and infections from stasis. Note: If stroke is not completed, activity increases risk of additional bleed (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Pad chair seat with foam or water-filled cushion, and assist patient to shift weight at frequent intervals.
-
Rationale: To prevent pressure on the coccyx and skin breakdown.
-
-
Set goals with patient and SO for participation in activities and position changes.
-
Rationale: Promotes sense of expectation of improvement, and provides some sense of control and independence.
-
-
Encourage patient to assist with movement and exercises using unaffected extremity to support and move weaker side.
-
Rationale: May respond as if affected side is no longer part of body and needs encouragement and active training to “reincorporate” it as a part of own body (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Provide egg-crate mattress, water bed, flotation device, or specialized beds, as indicated.
-
Rationale: Promotes even weight distribution, decreasing pressure on bony points and helping to prevent skin breakdown and decubitus formation. Specialized beds help with positioning, enhance circulation, and reduce venous stasis to decrease risk of tissue injury and complications such as orthostatic pneumonia (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
Position the patient and align his extremities correctly. Use high-top sneakers to prevent foot drop and contracture and convoluted foam, flotation, or pulsating mattresses or sheepskin.
-
Rationale: These are measures to prevent pressure ulcers.
-
Communication Deficits
A stroke can cause problems with communicating if there is damage to the parts of the brain responsible for language. These functions are controlled by the left side of the brain. As one side of the brain controls the opposite side of the body, many people who have communication problems after stroke also have weakness or paralysis on the right side of their body.
There are three primary types of communication deficits caused by a stroke:
-
Aphasia
-
Dysarthria
-
Dyspraxia
Aphasia (sometimes called dysphasia) means difficulty speaking or understanding language.
One may have problems with:
-
speaking
-
listening
-
reading
-
writing
-
dealing with numbers
-
understanding speech
-
thinking of words when talking or writing
How much trouble you have with aphasia depends on the type and severity of your brain injury. Not all strokes cause aphasia. About 20 percent of stroke survivors have a loss of speech and language ("Effects of Left-sided Stroke: Aphasia and Language Apraxia").
There are three main types of aphasia. Receptive aphasia is difficulty understanding what is being said. Expressive aphasia is difficulty expressing what you want to say. And Global aphasia is a combination of receptive and expressive aphasia and affects all or most of your communication.
Dysarthria is difficult or unclear articulation of speech that is otherwise linguistically normal. Most people describe it simply as slurred speech. The stroke survivor with dysarthria has no difficulty understanding what is being communicated to them and they have the ability to communicate but the way they are able to do this has been affected.
Symptoms of Dysarthria
-
Slurred speech.
-
Slow speech.
-
Speaking so softly it is difficult to hear.
-
Speech sounds breathless.
-
Saliva may drool out of the side of the mouth when speaking.
-
Control of lips, tongue and jaw affects the ability to form words or sounds.
-
Rhythm or tone of speech is affected.
-
Speech can sound rushed and incoherent.
-
Swallowing difficulties can mean there will be excess saliva in the mouth.
-
Speech can sound moist or gurgling
Dyspraxia is a condition that affects movement and coordination. Dyspraxia of speech happens when you cannot move muscles in the correct order and sequence to make the sounds needed for clear speech. The individual muscles you use to produce clear speech may be working well and you may have no weakness or paralysis, but you cannot move them when you want to, in the right order, or in a consistent way.
Expected outcomes for stroke survivors with speech/communication deficits are:
-
Identify and understand the communication problems.
-
Establish methods of communication that are effective in expressing one’s needs.
-
Use resources appropriately.

The nurse, physician, and speech-language pathologist will work together along with the rest of the team to assess, plan, and implement a plan to meet the communication goals of the patient
Nursing Interventions with Rationale:
-
Assess extent of dysfunction. Differentiate aphasia from dysarthria.
-
Helps determine area and degree of brain involvement and difficulty patient has with any or all steps of the communication process. Patient may have receptive aphasia or damage to the Wernicke’s speech area which is characterized by difficulty of understanding spoken words. He may also have expressive aphasia or damage to the Broca’s speech areas, which is difficulty in speaking words correctly, or may experience both. Choice of interventions depends on type of impairment. Aphasia is a defect in using and interpreting symbols of language and may involve sensory and/or motor components (inability to comprehend written and/or spoken words or to write, make signs, speak). A patient with dysarthria can understand, read, and write language but has difficulty forming and pronouncing words because of weakness and paralysis of oral musculature. Patient may lose ability to monitor verbal output and be unaware that communication is not sensible (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Listen for errors in conversation and provide feedback.
-
Feedback helps patient realize why caregivers are not understanding or responding appropriately and provides opportunity to clarify meaning (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Ask patient to follow simple commands (“Close and open your eyes,” “Raise your hand”); repeat simple words or sentences;
-
Tests for receptive aphasia (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Point to objects and ask patient to name them.
-
Tests for expressive aphasia. Patient may recognize item but not be able to name it (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Have patient produce simple sounds (“Dog,” “meow,” “Shh”).
-
Identifies dysarthria, because motor components of speech (tongue, lip movement, breath control) can affect articulation and may or may not be accompanied by expressive aphasia (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Ask patient to write his name and a short sentence. If unable to write, have patient read a short sentence.
-
Tests for writing disability (agraphia) and deficits in reading comprehension (alexia), which are also part of receptive and expressive aphasia (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Write a notice at the nurses’ station and patient’s room about speech impairment. Provide a special call bell that can be activated by minimal pressure if necessary.
-
Allays anxiety related to inability to communicate and fear that needs will not be met promptly (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Provide alternative methods of communication: writing, pictures.
-
Provides communication needs of patient based on individual situation and underlying deficit (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Anticipate and provide for patient’s needs.
-
Helpful in decreasing frustration when dependent on others and unable to communication desires (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
Talk directly to patient, speaking slowly and distinctly. Phrase questions to be answered simply by yes or no. Progress in complexity as patient responds.
-
Reduces confusion and allays anxiety at having to process and respond to large amount of information at one time. As retraining progresses, advancing complexity of communication stimulates memory and further enhances word and idea association (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Speak in normal tones and avoid talking too fast. Give patient ample time to respond. Avoid pressing for a response.
-
Patient is not necessarily hearing impaired, and raising voice may irritate or anger patient. Forcing responses can result in frustration and may cause patient to resort to “automatic” speech (garbled speech, obscenities) (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Encourage SO/visitors to persist in efforts to communicate with patient: reading mail, discussing family happenings even if patient is unable to respond appropriately.
-
It is important for family members to continue talking to patient to reduce patient’s isolation, promote establishment of effective communication, and maintain sense of connectedness with family (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Discuss familiar topics, e.g., weather, family, hobbies, jobs.
-
Promotes meaningful conversation and provides opportunity to practice skills (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Respect patient’s preinjury capabilities; avoid “speaking down” to patient or making patronizing remarks.
-
Enables patient to feel esteemed, because intellectual abilities often remain intact (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
-
Consult and refer patient to speech therapist.
-
Assesses individual verbal capabilities and sensory, motor, and cognitive functioning to identify deficits/therapy needs (Vera, "8 Cerebrovascular Accident (Stroke) Nursing Care Plans").
-
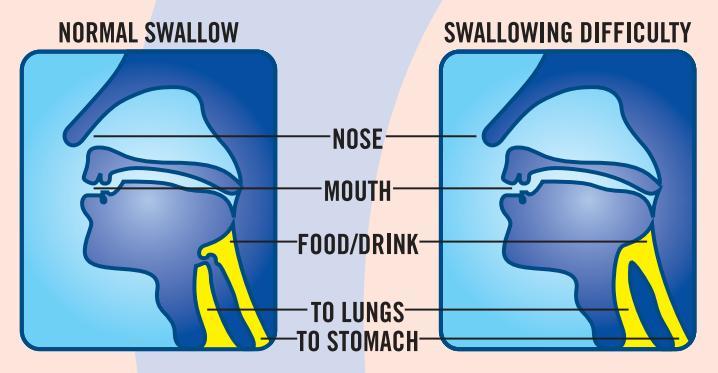
Swallowing Difficulties
Stroke survivors commonly have swallowing difficulties called dysphagia as a result of the stroke. Dysphagia may occur in up to 65 percent of stroke patients. If not identified and managed, it can lead to poor nutrition, pneumonia and increased disability. ("Swallowing Disorders After a Stroke").

(elderlycaresusj.blogspot.com/, 2013)
Speech-language pathologists are trained to test swallowing. The initial assessment will occur at the acute care hospital after the patient is medically stable. The first step is a bedside assessment of the patient’s swallow reflexes and is typically performed by the nurse. If the patient fails the swallow study, the SLP will be notified to perform a more detailed swallow study and the patient will remain NPO till the SLP makes a recommendation.
Efforts to make sure survivors with swallowing problems receive adequate nutrition are taken by the patient’s medical team. If it doesn’t appear safe for them to swallow anything by mouth, they may require tube feeding. The swallowing tests give the speech-language pathologist information to help create an individualized treatment plan to help patients regain their swallowing skills.
Treatment plans generally focus on exercises that improve coordination of muscle movements in the mouth and throat. A plan may also include techniques to help compensate for lost function. One technique is turning the head to one side to provide better airway protection. Another is taking only small sips of liquid so none splashes into the airway because of poor tongue control. Also, liquids may require thickening to reduce risk of aspiration. The speech-language pathologist will make their recommendation regarding the thickness of the liquids and the texture of the food based on their swallow study and continued assessment and tolerance of current diet. The SLP will determine when it is safe for the survivor to return to normal food and liquids ("Swallowing Disorders After a Stroke"). However, some survivors will remain of thickened liquids and modified foods, or tube feeding for the rest of their lives.
Although each treatment plan is unique and designed to meet specific needs, the following precautions may help the survivor swallow more safely:
-
Sit up straight any time you eat or drink.
-
Take small bites and sips.
-
Take your time.
-
Make sure you have cleared all the food from your mouth.
Expected outcomes of the treatment plan include:
-
Adequate nutrition
-
No aspiration
-
Follow swallowing techniques to improve outcomes and reduce risks
The rehabilitation nurse will continually monitor the patient for any signs of worsening dysphagia or aspiration. Signs include:
-
Coughing or choking while eating or drinking
-
Wet or “gurgly” voice quality during meals
-
Increased congestion after oral intake
-
Pocketing food
-
Drooling or inability to swallow own secretions
-
Tearing of the eyes when swallowing (may indicate silent aspiration)
-
Fatigue or shortness of breath when eating
Also, be aware that medication administration techniques may need to be altered relative to the patient’s swallowing difficulties. Meds may need to be crushed or given with pudding or apple sauce. If the patient has a feeding tube, then you may need to dissolve the meds and give via the feeding tube.
Stroke Prevention and Education
One of the rehabilitation nurse’s greatest responsibility to the stroke survivor and family is providing education that will help prevent or reduce the risk for another stroke. Did you know that of the almost 800,000 strokes that occur each year in the U.S., almost 200,000 of them are recurrent strokes ("Preventing Another Stroke")? Having a stroke simply puts one at a greater risk of having another one. That’s why it is so important to equip the stroke survivor as well as the family or caregivers with knowledge of prevention, symptoms, and risk factors.
Here are the facts:
-
Within 5 years of a first stroke, the risk for another stroke can increase more than 40%. (stroke.org)
-
Recurrent strokes often have a higher rate of death and disability because parts of the brain already injured by the original stroke may not be as resilient ("Preventing Another Stroke").
-
Within 5 years of a stroke, 24% of women and 42% of men will experience a recurrent stroke ("Preventing Another Stroke").
The good news is that there are steps you can take to prevent a recurrent stroke. It has been suggested that 80% of secondary strokes can be prevented by a combination of lifestyle changes and medical interventions ("Preventing Another Stroke"). First, the nurse can help the patient/family identify the risk factors that caused the first stroke. Once the causes have been identified and discussed, each risk factor needs to be addressed individually so that ways can be determined in preventing a recurrent stroke. The strategies will be different for each risk factor, but the goal is for the stroke survivor to make a plan and take control of his or her health ("Preventing Another Stroke").
Risk factors:
-
Stop smoking — it doubles risk for another stroke. Give patient/family a fact sheet on how to stop smoking ("Preventing Another Stroke").
-
Manage high blood pressure — high blood pressure is the most important modifiable risk factor for stroke. People who have high blood pressure have at least one and a half times the risk of having a stroke. Give patient/family a high blood pressure brochure ("Preventing Another Stroke").
-
Medications — Take medication as prescribed as this is critical to recovery and recurrent stroke prevention. Research shows that at least a quarter of stroke survivors stop taking one or more of their prescribed stroke prevention medications within the first three months — when the chance of having another stroke is highest—after having a stroke ("Preventing Another Stroke").
-
Manage high cholesterol — cholesterol or plaque build-up in the arteries can block normal blood flow to the brain and cause a stroke and increase risk of heart disease. Give patient/family a cholesterol brochure ("Preventing Another Stroke").
-
Keep diabetes under control — people with diabetes are up to 4 times as likely to have a stroke as someone who does not have the disease. Give patient/family a fact sheet about diabetes and stroke risk ("Preventing Another Stroke").
-
Manage atrial fibrillation (Afib) — Afib, a type of irregular heartbeat, increases your stroke risk five times, so it’s important to work with a healthcare professional to control it. Give patient/family an Afib fact sheet ("Preventing Another Stroke").
-
Eat a healthy diet — maintaining a diet low in calories, saturated fats, trans-fats and cholesterol helps manage both obesity and healthy cholesterol levels in the blood, which also reduces risk for stroke. Give patient/family a healthy eating fact sheet ("Preventing Another Stroke").
-
Increase physical activity — A recent study showed that people who exercise five or more times per week are less likely to have another stroke. Give handout on how to incorporate physical exercise into your daily routine ("Preventing Another Stroke").
-
Control alcohol use — some studies say that drinking more than 2 drinks per day may increase stroke risk by 50 percent. Discuss with patient/family about alcohol use and how it can best be controlled to prevent another stroke. Find out the risk factors that caused your first stroke. Take control and live your best life ("Preventing Another Stroke").

Conclusion
Strokes are the 5th leading cause of death in the U.S. and the leading cause of disability (“Prevention”). No one plans to have a stroke and when it occurs it is shocking and scary to the stroke victim as well as the family. Emotions such fear, depression, anger, and sadness will immediately creep in and rightfully so. And that’s why rehabilitation is so important. Not only can it improve the patient’s quality of life and outcome but through caring and empathy from the healthcare team, the fears and depression can be turned into confidence and hope. And seeing that transformation may be the greatest reward a rehab nurse can receive.
Although we have discussed the basics of stroke care in the rehabilitation setting, this is a field that continues to grow and adapt. There are many aspects of rehabilitation nursing not discussed in this article but this will give one a good foundation. As knowledge increases so will the application of that knowledge, and patient outcomes will continue to improve. Rehab Nurses play a vital role and some would say the most important part in the rehabilitation of the stroke victim. In fact, nurses spend more time with the patient than all the other disciplines combined, so it’s very important for the nurse to be equipped to meet the needs of the patient and family as well as equip them with knowledge so they can have a maximized life once they go home. But also remember, the whole team of healthcare providers is needed to cover the entire scope of rehabilitation and when working together, positive outcomes for the stroke victims are achieved.
References
"Difficulty Swallowing After Stroke (Dysphagia)." Life After Stroke. Stroke Connection Magazine, July-Aug. 2003. Web. 4 Aug. 2016.
Duncan, Pamela W., PhD, FAPTA,, Richard Zorowitz, MD, Barbara Bates, MD, John Y. Choi, MD, Jonathan J. Glasberg, MA, PT, Glenn D. Graham, MD, PhD, Richard C. Katz, PhD, Kerri Lamberty, PhD, and Dean Reker, Phd. "Management of Adult Stroke Rehabilitation Care." AHA/ASA-Endorsed Practice Guidelines. American Heart Association, 2016. Web. 3 Aug. 2016.
"Effects of Left-sided Stroke: Aphasia and Language Apraxia." Allina Health Patient Education, Understanding Stroke. Allina Health Patient Education Experts, 1 Feb. 2006. Web. 4 Aug. 2016.
"Frequently Asked Questions from the November 18, 2009, Training Webinar." New York State Department of Health. N.p., 18 Nov. 2009. Web. 19 Aug. 2016.
“Post-Stroke Rehabilitation." Know Stroke. National Institute of Health, Sept. 2014. Web. 2 Aug. 2016.
"Prevention." Together to End Stroke. American Heart Association, 2016. Web. 4 Aug. 2016.
"Preventing Another Stroke." National Stroke Association, Hope after Stroke. National Stroke Association, 2016. Web. 4 Aug. 2016.
"Signs and Symptoms of Stroke." National Stroke Association, Hope after Stroke. N.p., 2016. Web. 2 Aug. 2016
"Stroke Assessment Scales." The Internet Stroke Center. The Internet Stroke Center, Aug. 2011. Web. 19 Aug. 2016.
"Stroke: Hope Through Research." National Institute of Neurological Disorders and Stroke. National Institute of Health, 26 May 2016. Web. 18 Aug. 2016.
Vera, Matt, RN. "8 Cerebrovascular Accident (Stroke) Nursing Care Plans." NursesLabs. NursesLabs, 21 Aug. 2013. Web. 3 Aug. 2016.
Course Exam
Before you receive your certificate, you must complete the exam and achieve a score of % or higher. (You have unlimted attempts).
This exam is required by your state licensure.
Exam
Exam
We are required to delay the exam hours. Check back soon!
Exam
We are required to delay the exam until you have had time to view the course material. Please view the course first!
No Licenses on File
Please add a license to your account before you continue. Thank you!