Osteoarthritis
Osteoarthritis
Course Description
Osteoarthritis (OA) is the most common degenerative joint disorder with minimal inflammation, affecting 27 million people in United States. It affects women more than men and signs and symptoms increase with increasing age. In this course, we will consider its definition, risk factors, pathogenesis, signs and symptoms, laboratory findings, imaging, differential diagnosis, treatment, prognosis, economic impact and prevention.his course provides information regarding Osteoarthritis and includes content on diagnosis, treatment and other factors relevant to the clinical caregiver.
Accreditation Information: KLA Education Services LLC is accredited by the State of California Board of Registered Nursing, Provider # CEP16145.
Course Certification: Once you have completed this course, click on the “Print Certificate” option below to save or print your CE course certification. If you are not yet registered in a course plan with IvyLeagueNurse, please complete the registration and payment process so that you are able to log into your account and fully obtain your course certificate. Our affordable and unlimited one-year CEU plan starts at just $19.99.
Print Certificate Print Course
Course Objectives
Upon completion of this course, the course participant will be able to:
- Define and discuss a brief introduction to Osteoarthritis (OA)
- Discuss risk factors contributing to OA
- Define the pathogenesis of OA
- List 5 signs and symptoms of OA
- Recognize laboratory tests and imaging related to OA
- Identify differential diagnosis
- Discuss treatment/management of OA
- Discuss the prognosis of OA
- Discuss the economic impact of the disease
- Discuss prevention measures
Course Content
Definition and Introduction to Osteoarthritis
Osteoarthritis (OA) can be defined as:
“OA is a progressive degenerative joint disease characterized by loss of cartilage of joint, pain and stiffness” (Bhatia, et al. 2013; Fig. 1 &2).
OA is the most common type of arthritis and usually affects people above 60 years of age (Neogi, 2013). Therefore it is chiefly called as “disease of aging”. For the way of explanation, OA is a leading cause of joint pain and disability among older people due to progressive degeneration or breakdown of the joint involved which impacts many health outcomes (McDonough and Jette). However, OA shows minimal articular inflammation and no systemic symptoms. Pain is relieved at rest and morning stiffness is brief. Radiological findings in OA include narrowed joint space, osteophytes, bony cysts, and increased density of subchondral bone.
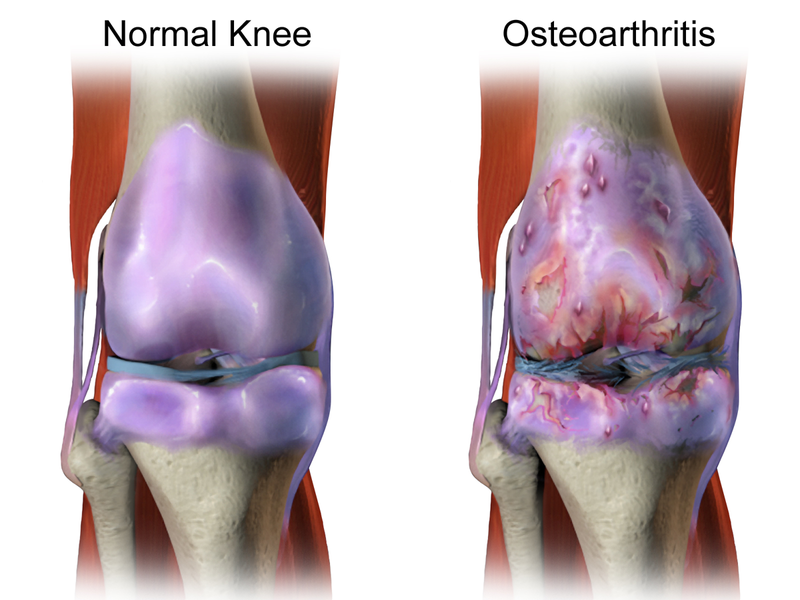
Figure 1: Swelling within and around the knee joint (Hunter Pain Clinic, 2016)
The patients who suffer from OA, 90% of them develop radiographic findings of OA in weight-bearing joints by the age of 40 (Papadakis, et al. 2017). Symptoms of OA increase as the patient ages. There are certain risk factors for the development of OA e.g. gender, obesity, and family history.
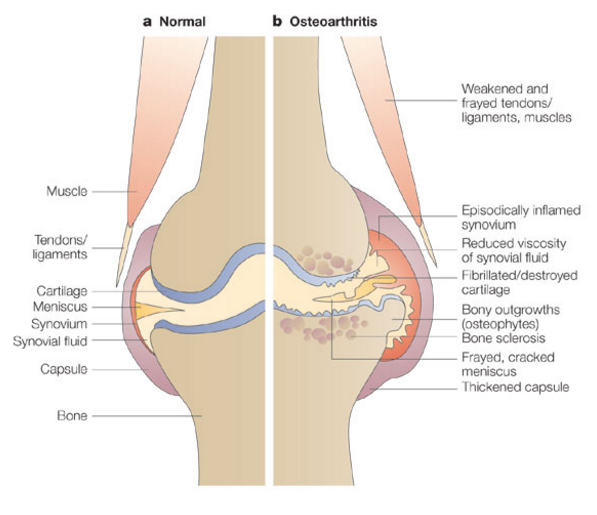
Figure 2: Drawing shows anatomy of normal and diseased knee joint and (Gavura, 2011)
Regarding arthritis, presence or absence of inflammation, the number of joints and specific sites involved affect differential diagnosis. These features help clinical diagnosis of the condition. For example, inflammation is a characteristic feature of rheumatoid arthritis while it is absent or minimal in case of OA (Fig. 3).
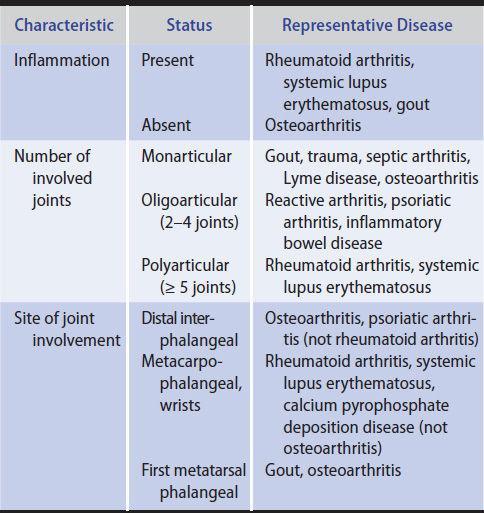
Figure 3: Diagnostic value of the joint pattern (Papadakis, et al. 2017)
Therefore, clinical examination of joint disease requires skills and expertise to reach the exact diagnosis.
Risk Factors of Osteoarthritis
The studies have reported that lifetime risk of developing symptomatic knee OA is about 45% in men and 47% in women (Murphy, et al. 2008). However, this risk is increased in the individuals who are obese. Risk factors of OA include person-level and joint-level risk factors. Person-level risk factors are gender, family history, obesity, metabolic syndrome, nutrition, bone density, and smoking. Joint-level risk factors include Joint/bone shape, injury, muscle strength, Joint load, occupation, leg length inequality, and physical activity (Allen and Golightly, 2015).
Person-Level Risk Factors
As mentioned above, person-level risk factors of OA include gender, age, family history, obesity, metabolic syndrome, nutrition, bone density, and smoking. These risk factors are described below:
Gender
Various studies have revealed that OA affects more females than males (Cho, et al. 2011). Additionally, OA is more severe in females as compared to that in males. It is hypothesized that hormones may play important role in the development of OA among females. Data collected from Women’s Health Initiative have demonstrated that women who take hormone replacement therapy (HRT) are less likely to require total knee or hip replacement as compared to those who do not take HRT (Cirillo, et al. 2006). Moreover, knee anatomy and kinematics may play important role in the development of knee OA.

Figure 4: Osteoarthritis affects more women than men (Cho, et al. 2011).
Age
As mentioned above, age is a recognized risk factor for osteoarthritis of all joints. Therefore, OA is called the “disease of aging”. As people grow older, various risk factors accumulate and certain biological changes take place which may affect the joint performance. Thinning of cartilage, weakened muscle strength, poor proprioception, and free radical damages make the joint prone to the wear and tear process. Studies have reported that 10% of men and 13% of women develop knee OA when they reach 65 years of age or above (Zhang and Jordan, 2010).
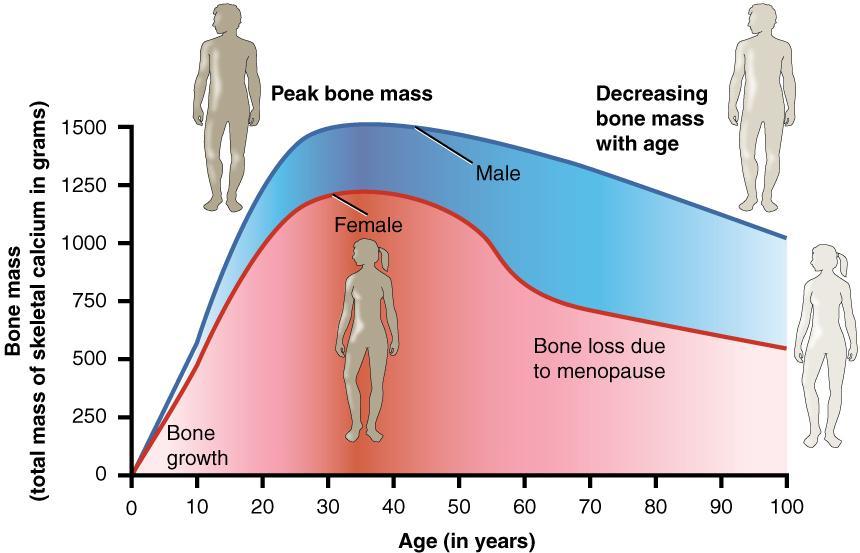
Figure 5: The relationship of age and bone mass (Creative Commons)
Family history or Genetics
Osteoarthritis is a complex and multifactorial condition where genetic components seem to have a strong contribution. Although the mechanism of genetic inheritance is not clear, family history should be considered in the near future. In this context, family history of OA may be a risk factor for the development of OA in the offspring. Several studies have identified various regions of chromosomes which may harbor susceptibility genes for OA (Loughlin, 2001; Chapman, et al. 2002). However, it is very important to recognize interaction between genetics and environmental stressors e.g. obesity, stress, injury, and joint articulation.
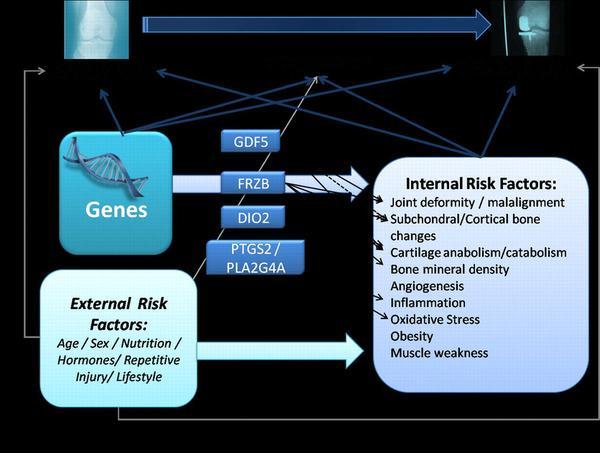
Figure 6: Internal and external risk factors for OA (Valdes and Spector, 2009)
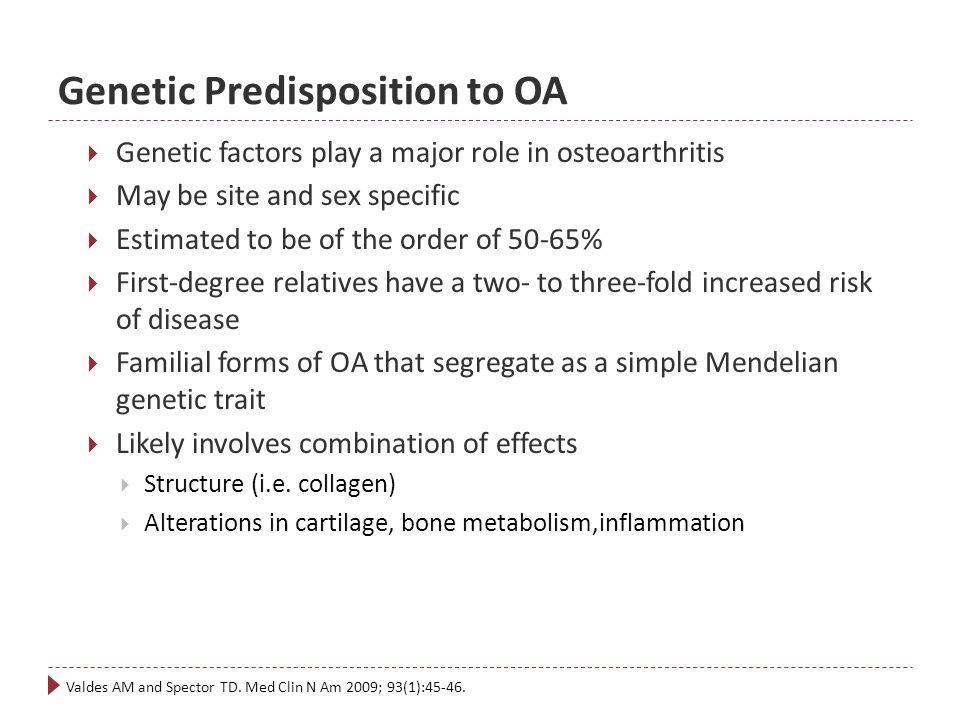
Figure 7: Some facts about OA (Valdes and Spector, 2009)
Obesity
Obesity is a recognized risk factor for OA. Excess adipose tissue interacts with hormones and alters articular cartilage metabolism. In this regard, the leptin system may have an association with metabolic abnormalities and risk for OA. Several studies have shown a significant association between obesity and OA (Cooper, et al. 2000). A study in Finland (Toivanen, et al. 2010) has reported a strong association of incident knee OA and basal metabolic rate (BMI). Similarly, Framingham study has also reported increased incident knee OA in those patients who had raised baseline BMI (Felson, et al. 1997).
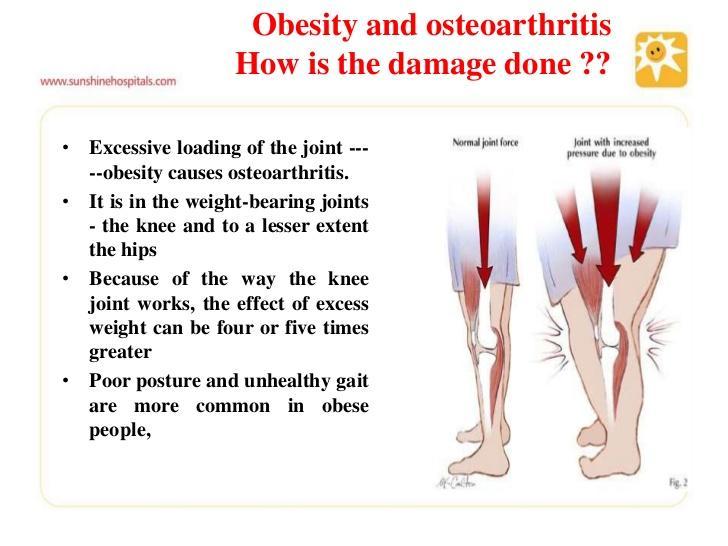
Figure 8: Excess weight, excess load and OA (Slideshare)
Adipose tissue produces bioactive products called adipocytokines or adipokines. The studies have suggested adipocytokines play a role in the development of OA due to their different patterns in the joint and circulating compartments (Chen, et al. 2006). Leptin, adiponectin, and resistin may cause degeneration of joint and subsequent OA (Sowers and Karvonen-Gutierrez, 2010).
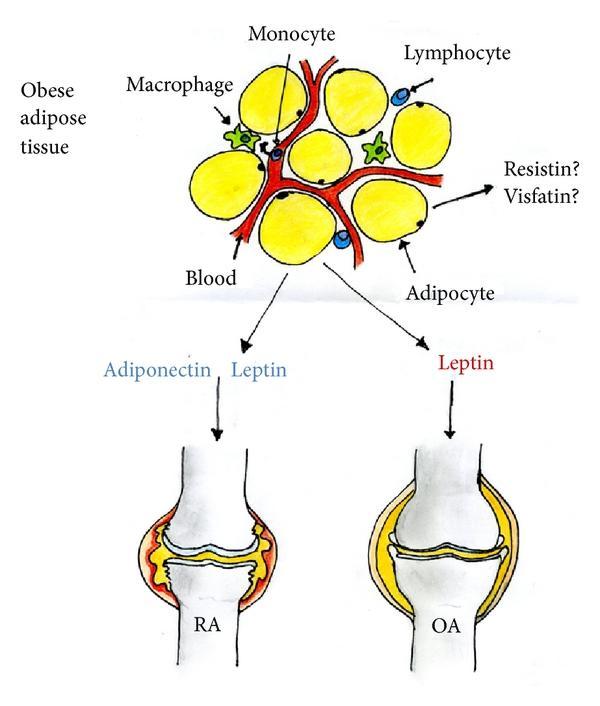
Figure 9: Adipocytokines are involved in the development of RA (rheumatoid arthritis) and OA (Source: www.hindawi.com)
Metabolic syndrome
Metabolic syndrome (MetS) refers to the cluster of conditions i.e. hypertension, obesity, dyslipidemia, and hyperglycemia which increase the risk of cardiovascular accident and diabetes. Hypertension compromises blood supply or nutrition to the joint through subchondral ischemia; dyslipidemia causes deregulation of cellular lipid metabolism in joint tissue; hyperglycemia damages cartilage by producing toxic internal environment; and adipocytokines inhibit cartilage matrix synthesis by inflammatory processes (Zhou, et al. 2012).
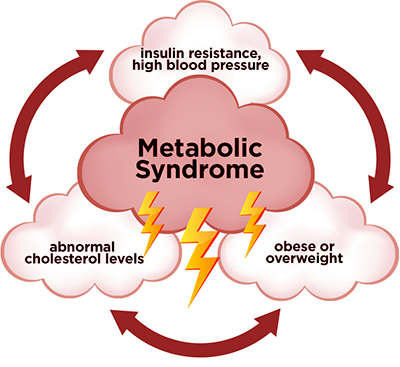
Figure 10: Metabolic syndrome
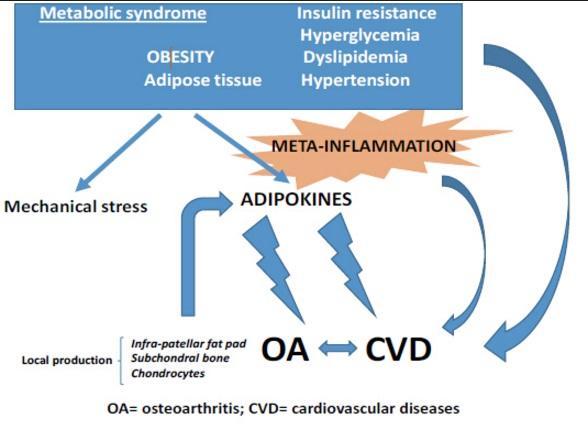
Figure 11: Metabolic syndrome and osteoarthritis (Source: www.ghrnet.org)
Nutrition
Nutrient deficiencies may play important role in the development of OA. Vitamin D deficiency leads to thin and brittle bones. Vitamin C deficiency is associated with enhanced progression of knee OA. Selenium deficiency leads to irregular bone formation, collagen abnormalities and decreased bone strength (Zhang and Jordan, 2010). However, the role of nutrient deficiencies and development of OA is unclear and controversial. Some studies recommend proper intake of vitamin D, vitamin C, vitamin K, selenium, fish, omega-3 fatty acid, and leafy vegetables to avoid OA. Moreover, high cholesterol has strong association with OA; so it is better to be avoided. Mediterranean diet is associated with better quality of life, reduced pain and disability, and depressive symptoms (Veronese, et al. 2016). In this regard, more studies, to large extent, are required to identify the relationship between nutrition and OA.
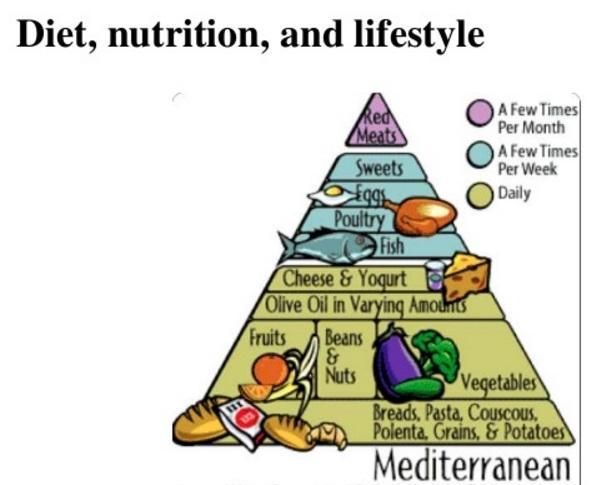
Figure 12: Mediterranean diet is associated with better quality of life (Veronese, et al. 2016)
Bone Density
High bone density or bone mineral density (BMD) is one of the risk factors for OA (Neogi and Zhang, 2013). Studies have reported that prevalence of knee OA is more common among people with high bone density as compared to the controls (Hardcastle, et al. 2014). As high bone mass is a lifelong genetic trait, it supports the occurrence of OA in old age. Moreover, it has been suggested that increased bone density leads to subchondral bone sclerosis and subsequent hypertrophic OA (Allen and Golightly, 2015).
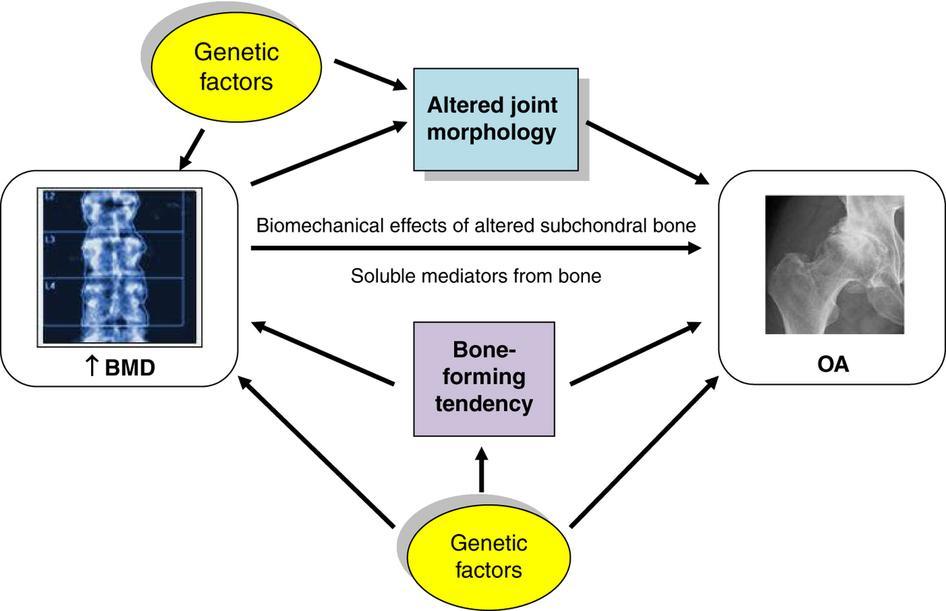
Figure 13: Association between bone mineral density (BMD) and OA (Hardcastle, et al. 2015)
Smoking
Most likely, smoking has an inverse relationship with OA. Recent meta-analyses reached the conclusion of inverse relation except in cohort studies. Smoking offers moderate protection against knee or hip OA. However, the patients who smoke report painful OA (Hui, et al. 2011).

Figure 14: Smoking may protect against OA
On the other hand, long-term smoking shows no advantage against OA. Therefore, large trials are required to identify the exact relationship between smoking and OA.
Joint-Level Risk Factors
As mentioned above joint-level risk factors of OA include Joint/bone shape, injury, muscle strength, Joint load, occupation, leg length inequality and physical activity. These risk factors are described below:
Joint/bone shape
Bone or joint shape plays important role the pathogenesis of OA. Femoroacetabular impingement and acetabular dysplasia are involved in the development of hip OA. Several anatomical and structural variations affect joint performance and joint disorders. For example, increased hip height center, increased valgus neck-shaft angle, increased abductor angle, and decreased femoral offset prone to knee OA (Boissonneault, et al. 2014). Large Q-angle in women leads to more OA among women than in men.
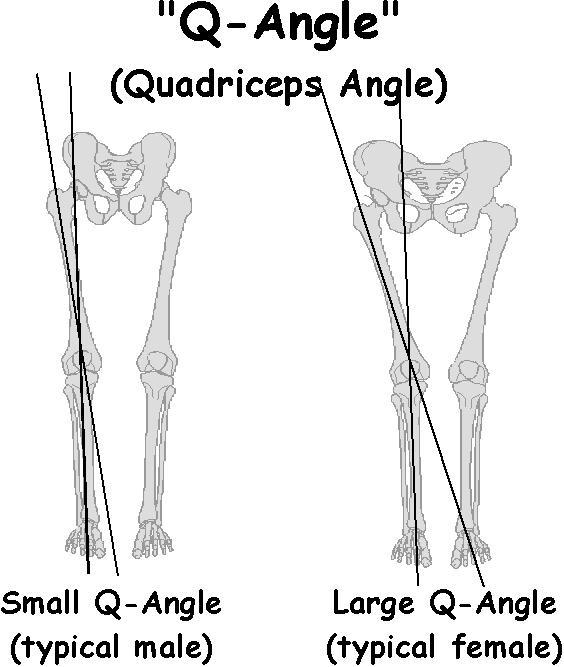
Figure 15: Wider Q-angle in women causes more OA in women
Injury
Injury to the joint (especially knee and ankle joints) is a recognized risk factor for the development of OA. These injuries may be in the form of meniscal damage, rupture of anterior cruciate ligament (ACL), or direct trauma to cartilage. Trauma to joint causes acute post-traumatic arthritis and osteoarthritis as a chronic complication. In United States, approximately 900,000 cases of OA are reported of which 12% are contributed by post-traumatic OA (Brown, et al. 2006). Recently, a systematic review have demonstrated that the patients with ACL deficiency plus knee reconstruction show altered synovial fluid biomarkers indicative of OA as compared to controls (Harkey, et al. 2015). Moreover, injury accelerates the process of disease.
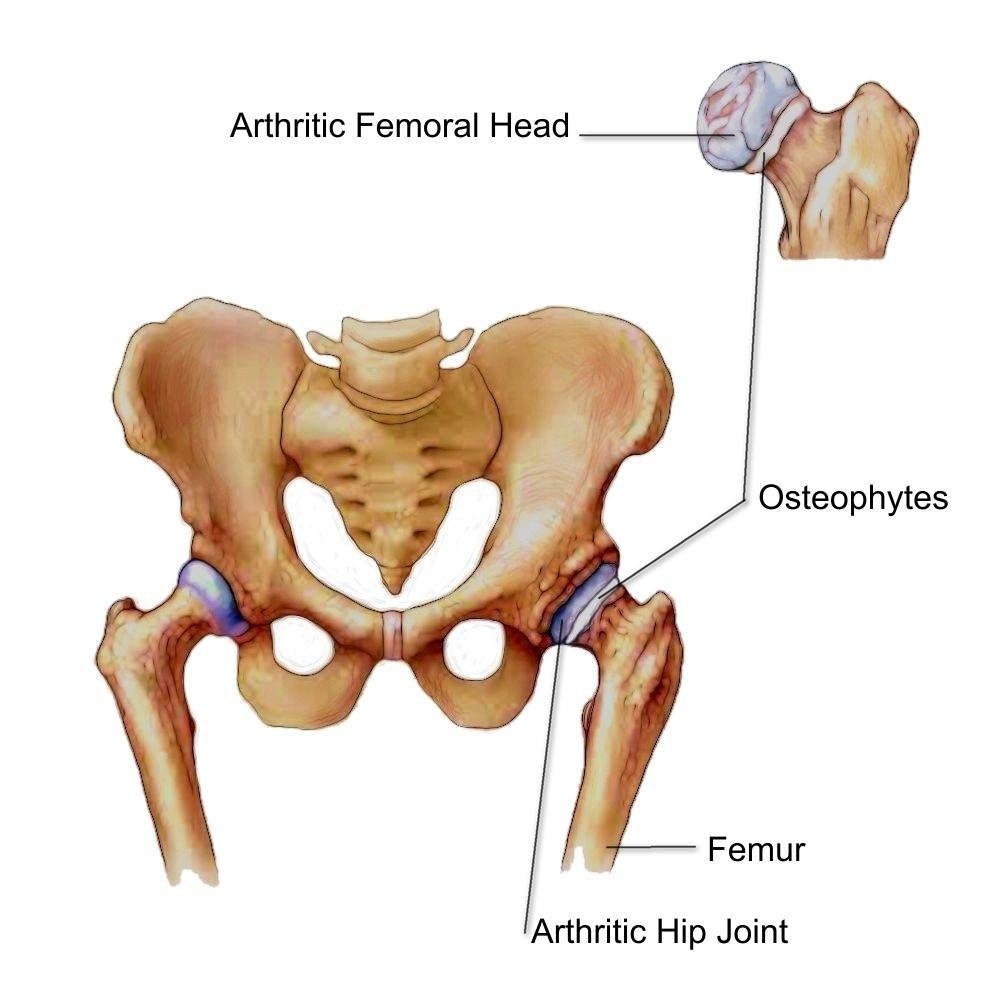
Figure 16: Posttraumatic osteoarthritis develops as benign degradation of joint, especially in sports injuries (Source: www.epainassist.com)
Muscle strength
The exact role of muscle strength in the pathogenesis of OA is still to be evaluated. It is suggested that weakened muscles may be a risk factor for the onset and progression of OA. Isometric knee extensor and flexor strength has been reported lower in symptomatic as compared to asymptomatic knee OA (Allen and Golightly, 2015).
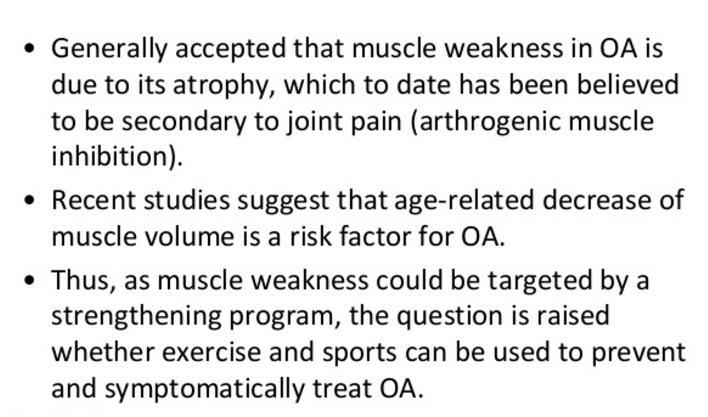
Figure 17: Muscle weakness in OA (Source: Slideshare)
Joint load
Studies have revealed that increased joint load is a risk factor for OA. Obesity is one of the documented risk factors for OA as overweight increases joint and subsequent joint damage (Lee et al. 2015). Additionally, it has been suggested that obesity related systemic and metabolic factors may play important role in the inflammatory process of OA. In one of the studies, it has been stated that obesity may contribute to 27% and 69% cases of hip arthroplasty and knee arthroplasty, respectively (Grazio & Balen, 2009). Therefore, weight reduction may play a very important role in the prevention of OA.
Occupation
Occupations with a heavy physical work load is a common risk factor OA. Other occupational factors which contribute to OA include kneeling, regular stair climbing, crawling, bending and repetitive movements (Yucesoy et al. 2015). The individuals who spent a lot their time in knee-straining positions (floorlayers, carpenters, and compositors) and those who work in construction industry (firefighting, agriculture, fisheries, and mining) are at increased risk of developing knee OA.

Figure 18: Repetitive body movements contribute to OA (Source: www.xarxalocaldintercanvi.blogspot.com)
Leg length inequality
Leg length inequality or leg length discrepancy (LLD) affects about 90% of population, 5.2 mm being the mean discrepancy (Knutson, 2005). LLD is also known as short leg syndrome. This discrepancy leads to unequal or abnormal loading of joints of the lower extremities. LLD can be structural, functional, or environmental. In structural discrepancy, side-to-side differences are observed. In functional discrepancy, biomechanical abnormalities in joint function are noted. Environmental LLD is a type of functional discrepancy where individuals run on sloping surfaces for long periods of time, for example, runners. LLD or unequal stress on the joints causes abnormal loads on the joint cartilage, leading to damaged cartilage and subsequent OA development (Murray & Azari, 2015). However, this issue of LLD is still to be understood on a large scale, and the combination of clinical and radiological assessment may offer precise results.
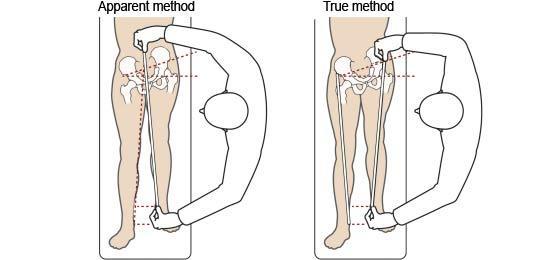
Figure 19: Measuring limb length (Source: www.physio-pedia.com)
Physical activity
Insufficient evidence is available about physical activity whether it has a role in the development of OA or not. In other words, some of the studies consider high physical activity as a risk factor for OA while others do not. However, it is documented that vigorous activity is positively associated with knee replacement therapy (Wang et al. 2011). It can be suggested that regular exercise should be encouraged in the individuals without any joint injury.
Pathogenesis of Osteoarthritis
OA is one of the complex disorders that involve genetic as well as environmental components. Occupation related repetitive adverse of loading of joints is an important predisposing factor among farmers, minors or athletes. However, recreational sports have no link as predisposing factor until a significant trauma of the joints occurs. Other factors including abnormal load distribution within the joint, obesity, and various genetic factors may predispose someone to the development of OA.
Major alterations in cartilage structure are the hallmark of OA. Derived from chondrocytes, metabolically active cells produce nests. Initially, a balance between the production of matrix components and degradation of the major structural components of cartilage is maintained. Eventually, the process of degradation of the matrix becomes more than that of production, leading to decreased concentration of aggrecan in the matrix making the cartilage vulnerable to loading injury. Deep vertical clefts develop as a result of fissuring of the cartilage surface. Localized chondrocyte death leads to reduced cartilage thickness. Additionally, calcium pyrophosphate and calcium phosphate crystals get deposited in the abnormal cartilage.
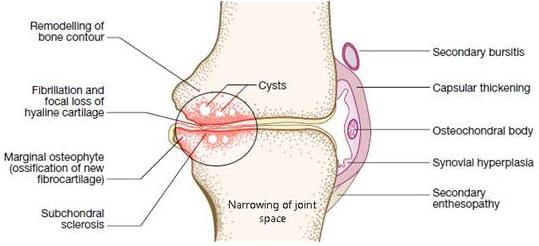
Figure 20: Narrowing of joint space (Source: www.yourdiagnosis.com)
OA does not only involve the cartilage, it also affects the subchondral bone and leads to osteosclerosis and subchondral cyst formation. Fibrocartilage at the joint margin undergoes endochondral ossification which results in osteophyte formation. Bone remodeling and cartilage thinning alters the shape of joint, increasing the surface area. Studies have revealed that the patients with OA also have higher bone mineral density (BMD) values at the sites other than the involved joints which probably relates to osteophyte formation. Higher BMD values may reflect that common signaling pathways regulate bone and cartilage metabolism.
Additionally, inflammatory changes and synovial hyperplasia occurs in the patients with OA. Chondroid metaplasia may be seen in the form of osteochondral bodies formed within the synovium. The outer capsule thickens and contracts, and the muscles surrounding the joint begin to waste.
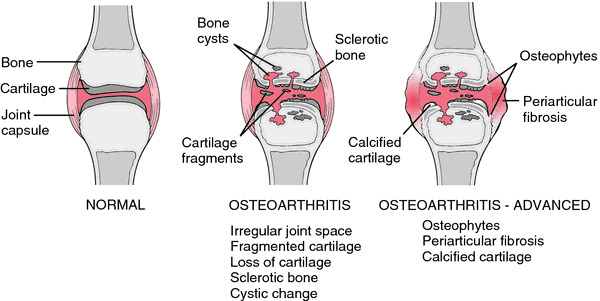
Figure 21: Schematic presentation of the pathologic changes in OA (Source: www.thefreedictionary.com)
Signs and Symptoms of Osteoarthritis
Pain
The major presenting complaint of OA is pain and functional restriction over the age of 45. However, more often the patients present after the age of 60. The exact reason of pain is still unknown; however, it may be described on the basis of increased pressure in subchondral bone, trabecular microfractures, capsular distension, and low grade synovitis (Walker et al. 2014). Others reasons of pain may include bursitis and enthesopathy secondary to abnormal joint mechanics. The characteristics of pain in OA are:
-
Insidious onset over months and years
-
Variable of intermittent pain over time – good days, bad days
-
Mainly related to movement and weight-bearing, relieves on rest
-
Brief morning stiffness (<15 minutes) and brief (<5 minutes) gelling after rest
-
One or few joints are involved
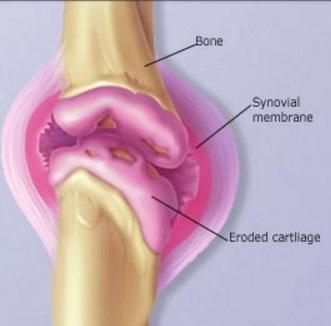
Figure 22: Pain is the major symptom of OA (Source: www.webMD.com)
Functional restriction
Functional restriction imposes a substantial impact on the daily life of the patients. Pathology (biochemical or physiological abnormalities) leads to impairments (functional limitations) and then limitations or disability (McDonough & Jette, 2010). In many patients with OA, functional restriction accounts for an equal problem with the pain. Clinical findings vary with the severity and site of the disease. Various factors like age, body mass index, exercise, comorbid conditions, and depression are involved in the functional disability in the patients with OA. Restricted movements in OA are caused by capsular thickness or blocking by osteophytes.
Pathology → Impairments → Disability

Figure 23: OA and functional restriction (Source: www.niams.nih.gov)
Stiffness
Morning stiffness is common in patients with OA (<15 minutes). It usually occurs after sleep or rest. It may occur throughout the whole day during the periods of inactivity (<5 minutes) (Walker et al. 2014).
Crepitus
Rough articular surfaces of the joint produce coarse, crackling, or grating sensation named as crepitus.
Swelling/Effusion
Accumulation of excess fluid in the joint space is called effusion which is observed clinically as a swelling around the joint. Synovitis is also an important feature of the pathogenesis of OA.
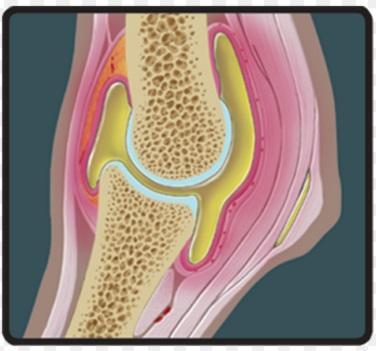
Figure 24: Synovitis in OA (Source: www.equinelegend.com)
Bony outgrowths/Osteophytes
The patients with OA may develop bony protuberances or outgrowths termed as osteophytes or bony spurs. Osteophytes are actually the outgrowth of cartilage which subsequently undergoes endochondral ossification.
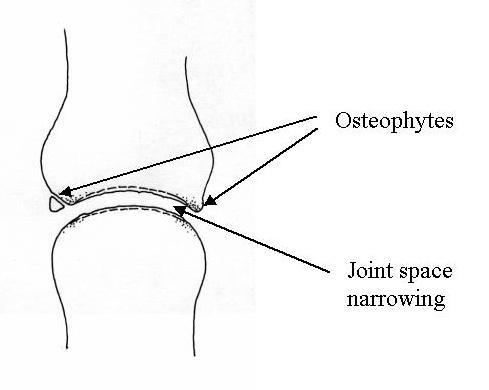
Figure 25: Osteophytes in OA (Source: http://www.emedicinehealth.com)
Muscle weakness
Muscle weakness has been documented in the patients with OA. Knee joint OA is associated with weakness of quadriceps muscles. This weakness is called arthrogenic muscle inhibition (AMI) which may lead to muscle atrophy as well.
Specific Joints
OA does not involve all the joints equally; that is why it is usually called asymmetrical. Most often, it affects fingers, knees, hips, and spine.
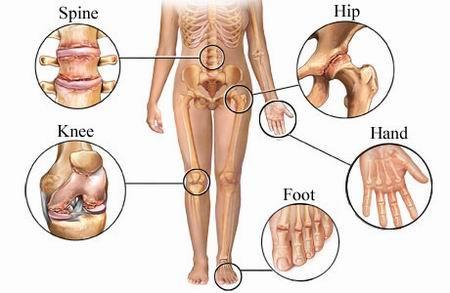
Figure 26: Joints commonly affected in OA (Source: www.doctortipster.com)
Generalized Nodal Osteoarthritis
It is the most common form of OA. It may be asymptomatic or may be with characteristic features like pain, stiffness, and swelling. Characteristics of generalized nodal OA include:
-
Polyarticular finger interphalangeal joint OA
-
Heberden’s nodes ± Bouchard’s nodes
-
Female > Male
-
Peak onset in middle age
-
Good functional outcome of hands
-
Predisposition to OA at other joints
-
Affected joints are enlarged due to osteophytes formation
-
Strong genetic predisposition
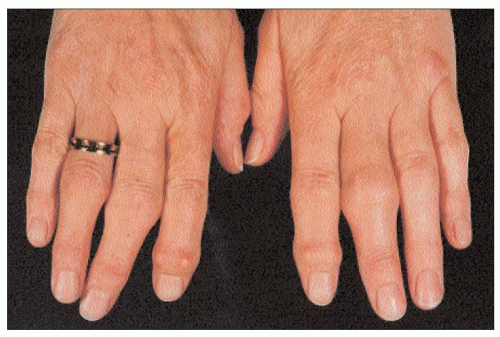
Figure 27: Nodal OA of the hands: Heberden’s nodes at the distal interphalangeal (DIP) joints & Bouchard’s nodes at the proximal interphalangeal (PIP) joints (Source: www.musculoskeletalkey.com)
Knee Osteoarthritis
Knee OA targets patellofemoral and medial tibiofemoral compartment of this region. However, it affects the whole joint eventually. Knee OA can be symmetrical, a part of nodal OA, or an isolated case. The pain is mostly observed in the same compartments where the disease targets. Baker’s cysts or popliteal cyst may cause pain on the posterior aspect of the joint. Examination of the knee joint may reveal:
-
A jerky, asymmetric gait
-
A varus, or less commonly valgus
-
Joint-line or periarticular tenderness
-
Weakness and wasting of quadriceps muscle
-
Restricted flexion or extension
-
Bony swelling around the joint-line

Figure 28: A varus in knee OA (Source: www.goudelis.gr)
Hip Osteoarthritis
Most commonly, hip OA targets superior aspect of the hip joint and usually progresses with superolateral migration of femoral head and has poor prognosis. Central OA usually affects women where cartilage in the centre is lost. Associated with generalized nodal OA, central hip OA often presents as bilateral manifestation. It has better prognosis as compared to the superior hip OA.
The symptoms in hip OA are correlated best with the corresponding radiological changes. The hip is the deepest in the anterior groin while lateral hip pain is worse lying on the left side.
The examination of hip can reveal the following:
An antalgic gait
Weakness and wasting of quadriceps and gluteal muscles
Pain and movement restrictions
Anterior groin tenderness
Fixed flexion, external rotation deformity of the hip
Ipsilateral leg shortening

Figure 29: Arthritic hip joint (Source: www.physiofix.com.au)
Spine Osteoarthritis
Spine OA usually affects cervical and lumbar regions. It may present as an isolated manifestation or as a part of generalized nodal OA. It typically presents as low back or neck pain. The pain can, however, radiate to arms, buttocks, or legs. On examination:
-
The range of movements may be restricted; loss of lumbar lordosis is typical.
-
The straight leg-raising test may be positive.
-
Neurological signs may include the manifestations of spinal stenosis and nerve root compression.
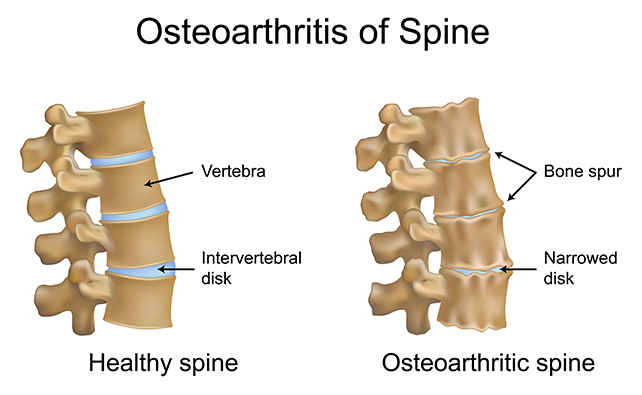
Figure 30: OA of spine (Source: www.stkildaosteopathy.com.au)
Early-onset OA
Early-onset OA refers to the condition when typical features of OA present before the age of 45. Most often, a single joint is involved with strong history of trauma. However, specific cause must be ruled out especially when typical sites of OA are not involved. Causes of early-onset OA include:
-
Juvenile idiopathic arthritis
-
Metabolic or endocrine disease
-
Spondylo-epiphyseal dysplasia
-
Late vascular necrosis
-
Neuropathic joint
-
Kashin-Beck disease
Erosive Osteoarthritis
It is rare with more prolonged symptoms, overt inflammation, and disability; and has a worse outcome compared to nodal OA. It can be differentiated from generalized nodal OA on the basis of:
-
Preferential targeting of PIP joints
-
Subchondral erosions on x-rays
-
Occasional ankylosis of the affected joints

Figure 31: Erosive OA (Source: www.posterng.netkey.at)
Investigations for Osteoarthritis
Diagnosis of OA is most often clinical; however, plain radiology may help reach the diagnosis.
Imaging/X-rays: An x-ray of the affected joint should be performed. It can show one or more typical features of OA e.g. marked loss of joint space, marginal osteophyte formation, sclerosis of subchondral bone, varus deformity, and cysts formation.

Figure 32: Joint space narrowing of a knee joint (Source: www.blog.rodandmolly.com)

Figure 33: Extensive osteophytosis (Source: http://www.discoverymedicine.com)

Figure 34: Gull wing and saw tooth appearance in erosive OA (Source: http://www.discoverymedicine.com)
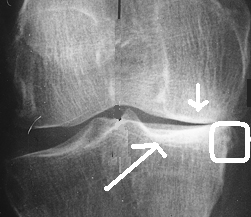
Figure 35: Knee OA with joint space narrowing (short arrow), subchondral sclerosis (long arrow) and osteophyte (circled) (Source: www.orthopaedicsone.com)
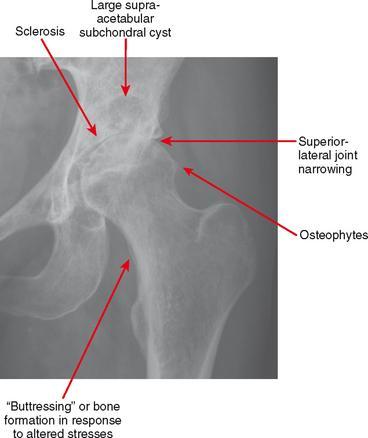
Figure 36: Butteressing, osteophyte formation and subchondral sclerosis in hip OA (Source: http://radiologykey.com)
A plain x-ray not only helps making diagnosis, it also helps assessing the severity of the disease while deciding for joint replacement therapy. Non-weight-bearing posteroanterior views of the pelvis are enough to assess hip OA. The patients with suspected knee OA should get a standing anteroposterior radiograph in order to evaluate tibiofemoral cartilage loss and fixed skyline view for patellofemoral involvement. Disc space narrowing and osteophytes can be seen in spine OA. An MRI should be performed if nerve root compression or spinal stenosis is suspected.
Other tests: OA does not cause elevation of erythrocyte sedimentation rate (ESR), or changes in routine biochemistry, haematology, and autoantibody tests. Synovial fluid examination is non-inflammatory. However, the synovial fluid may be viscous with low cell count. Sometimes incidentally, radioisotope bone scans run for other reasons may show increased uptake in the joints with OA due to increased bone remodeling. Unexplained early-onset OA may require further investigations in order to rule out suspected underlying causes. In this case, xrays may show avascular necrosis, widening of joint spaces in acromegaly, multiple cysts, chondrocalcinosis in haemochromatosis, and disorganized architecture in neuropathic joints.
Differential Diagnosis
Minimal articular inflammation and absent systemic manifestation can be confused with other conditions. However, distribution of joint involvement can distinguish it from other arthritic conditions. For example, OA chiefly affects DIP and PIP while spares wrist and MCP joints. On the other hand, rheumatoid arthritis (RA) chiefly affects the wrist and MCP joints and spares DIP. Additionally, joint enlargement is bony-hard and cool in OA while spongy and ward in RA (Papadakis et al. 2017).
-
Crystalline arthropathies (i.e. gout and pseudogout)
-
Inflammatory arthritis (e.g. rheumatoid arthritis)
-
Seronegative spondyloarthropathies (e.g. psoriatic arthritis and reactive arthritis)
-
Septic arthritis or postinfectious arthropathy
-
Fibromyalgia
-
Tendonitis
There are various other diseases which can cause secondary OA and, therefore, these conditions must be considered if they exist on the background:
-
Chondrocalcinosis
-
History of joint trauma
-
Metabolic bone disorders
-
Hypermobility syndromes
-
Neuropathic diseases
Management
So far, the management of OA relies on symptomatic relief. In other words, there is still no cure to OA except managing the risk or predisposing factors of the disease progression. Osteoarthritis Research Society International (OARSI) and the American Academy of Orthopaedic Surgeons (AAOS) consider physical measures, drug therapy, and surgery as the mainstay of OA management (Zgang, et al. 2016). Hence, the management of OA can be divided into three parts: non-pharmacological and preventive strategies, pharmacological therapie,s and surgical interventions. Here, we will discuss these options one by one:
Non-Pharmacological and Preventive Strategies
Education, physical therapy and weight loss are major pillars of non-pharmacological and preventive measures.
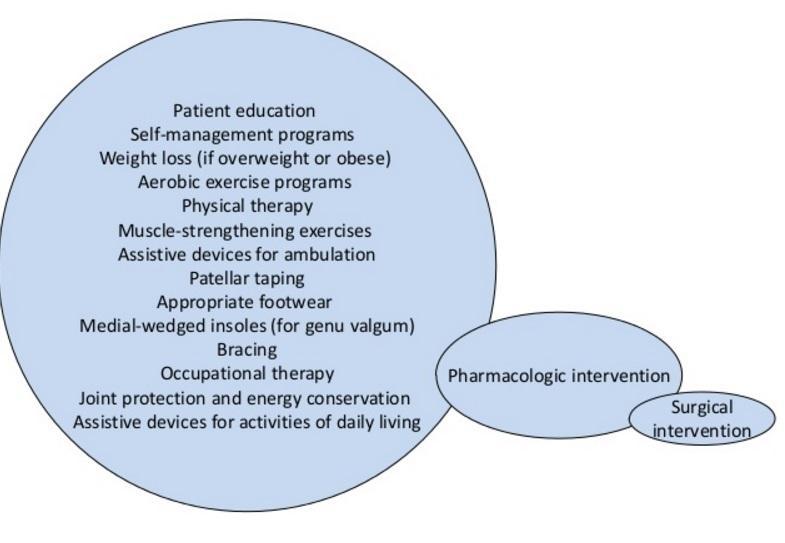
Figure 37: Management of OA (Source: www.pt.slideshare.net)
A number of studies have revealed the significant role of patient education, exercise, and weight loss in order to reduce pain and improve general health (Anandacoomarasamy, 2010). However, in this regard, the recommendations depend on various factors such as common sense, economical status, and expert opinion.
Patient Education: The patients suffering from OA may feel frustrated, dependent, and even depressed. Actually, the reason is having the sense of long-term disability and being dependent on others. These feelings may discourage the patients, reducing the compliance to the treatment. In this context, if the patients are educated that they have some control over their chronic condition, the outcome is improved. Therefore, researchers have developed self-management approaches in the form of exercise training, coping skill training, social support, and patient education.
Exercise and Weight Loss: Being a recognized risk factor of OA, obesity plays an important role in the pathophysiology of OA. Therefore, studies have shown that weight reduction helps people with osteoarthritis in terms of pain relief. Several studies have supported that weight loss improves pain and function among the patients with OA. For example, Messier et al. (2004) conducted “the Arthritis, Diet, and Activity Promotion Trial (ADAPT)” including 316 overweight patients for 18 months and concluded that modest weight loss led to significant pain relief and physical function. Similarly, Christensen et al. (2005) reported that weight reduction of 10% offers 28% improvement in physical function in the patients with knee OA.
Exercise improves pain and function in the patients suffering from arthritis. However, exercise therapy should be individualized and patients-centered on the basis of age and comorbidities. In this context, home or grouped exercise therapies are equally effective; however, compliance is the key factor for the improvement. Hydrotherapy is also a useful addition to the exercise therapy. Additionally, correcting malalignment and using walking sticks can improve function and reduce pain; however, data is sparse in this regard.
Assistive devices can help the patients with OA of the hand. The patients with mild to moderate disease should attend regular exercise programs. Splinting is beneficial for the patients with first carpometacarpal joint OA.

Figure 38: Physiotherapy for OA (Source: www.sciencedaily.com)
Pharmacological Therapy
Pharmacotherapy is the most common therapy used for the patients with OA. It aims at relieving pain (analgesics) and reducing inflammation (anti-inflammatory agents). Traditional drugs, new agents, and regenerative therapy are the most investigated areas in osteoarthritic therapeutics. Traditional drugs for OA only offer symptomatic relief and do not reverse any damages. On the other hand, new drugs with fewer side effects are underway. Regenerative therapy is also promising to offer significant results.
Traditional Drugs: Most often, there are mainly five types of medications used to treat OA. These five medications are acetaminophen, NSAIDS (non-steroidal anti-inflammatory drugs), opioid painkillers, SNRIs (serotonin-norepinephrine reuptake inhibitors), and intra-articular injections.
Acetaminophen: It is an essential over-the-counter medicine used for fever and pain relief. It is recommended as first-line oral drug therapy for the mild OA due to its effectiveness and safety. Its recommended dose for OA is 2.6-4 grams per day per oral. ACR and OARSI recommend Acetaminophen, up to 4 grams per day, for the initial treatment for mild-to-moderate knee or hip OA (Zgang, et al. 2016). However, due to its side effects on liver, FDA (2011) has put limitation on its dose in combination with other molecules i.e. no >325 mg per dose in combination.
Non-Steroidal Anti-inflammatory Drugs (NSAIDs): NSAIDs are potent analgesics and anti-inflammatory drugs which have long been used in the treatment of OA. Although NSAIDs are more effective than acetaminophen, they have greater toxic effects. NSAIDs inhibit an enzyme called cyclooxygenase (COX), reducing the production of prostaglandins. COX exists in two forms i.e. COX-1 and COX-2. COX-1 is continuously found in many cells while COX-2 is expressed in inflammatory tissues. Most of the time, NSAIDs inhibit both forms of COX and thus inhibit their beneficial effects, as well as cause adverse effects. Gastric ulceration, perforatio,n and hemorrhage are the most common adverse effects of NSAIDs. These agents may also perforate lower gastrointestinal tract and may aggravate inflammatory bowel disease. The risk of side effects with NSAIDs is increased with:
-
Long-term use of NSAIDs
-
Higher doses of NSAIDs
-
Concomitant use of corticosteroids or blood thinning agents (anticoagulants)
-
Previous history of peptic ulcer
-
Presence of rheumatoid arthritis
-
Alcoholism
-
Age above 70
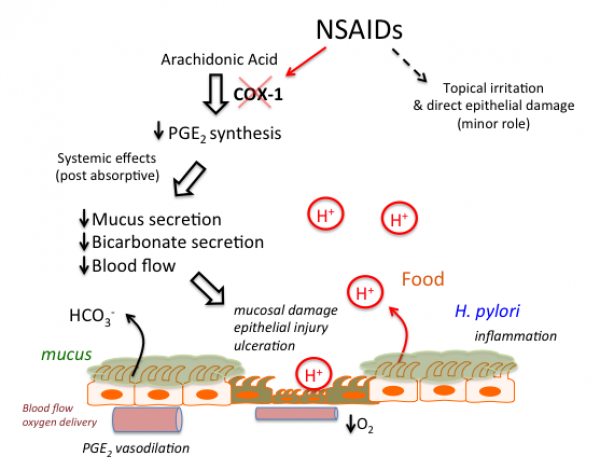
Figure 39: Gastrointestinal side effects of NSAIDs (Source: www.tmedweb.tulane.edu)
The side effects can be reduced by using omeprazole 20 mg daily. On the other hand COX-2 inhibitors (e.g. celecoxib) may cause lesser side effects as compared to COX-1 inhibitors; however, it increases cardiovascular risks. Apart from gastrointestinal side effects, NSAIDs also cause:
-
Renal toxicity – interstitial nephritis, prerenal azotemia, nephrotic syndrome, hypertension
-
Hyperkalemia – hyporeninemic hypoaldosteronism
-
Platelet dysfunction - increased bleeding time
Topical NSAIDs are superior to placebo and have lesser side effects.
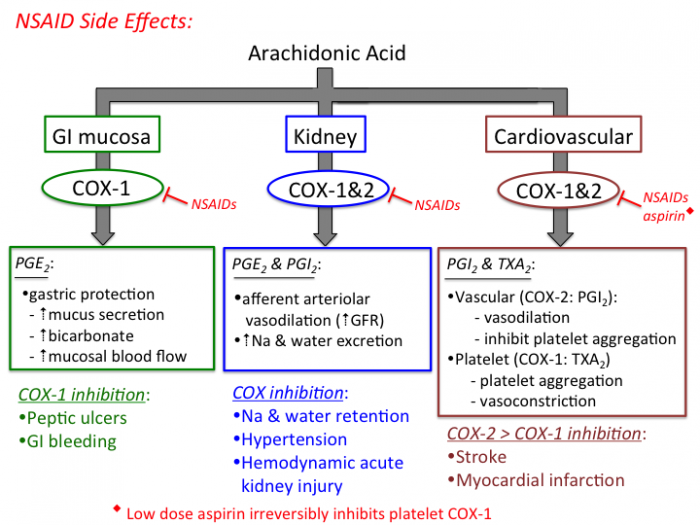
Figure 40: Side effects of NSAIDs (Source: www.tmedweb.tulane.edu)
Opioid Analgesics: Opioid analgesics are used when acetaminophen and NSAIDs fail or contraindicated to manage OA (Zhang, et al. 2008). Due to the risk of opioid abuse and side effects (e.g. headache, sleeplessness, constipation, nausea and vomiting), low doses are recommended.
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs): These agents are used to treat depression and mood disorders. FDA has approved duloxetine for the patients with musculoskeletal pain. SNRIs may be efficacious agents for the patient with OA who cannot take other medicines.
Intra-articular Injections: Intra-articular injections can be considered in those who do not respond to oral analgesics and anti-inflammatory agents. Two types of intra-articular injections are used: corticosteroid and hyaluronic acid. Triamcinolone (20-40 mg) in the patients with knee or hip OA may decrease the demand for pain-killers. This injection can be repeated four times per year. Similarly, injection of sodium hyaluronic acid moderately reduces the symptoms of OA.
New Drugs
Unsatisfactory effects and side effects of traditional drugs provoked the development of newer drugs. Newer drugs for OA include bone morphogenetic protein-7, interleukin-1β, β-nerve growth factor, fibroblast growth factor, platelet-rich plasma, human serum albumin and methotrexate. Most of these drugs are being tested or are under-developmental processes.
Regenerative Therapy
Cell-based therapy and tissue engineering may be applied to repair the damaged cartilage which reduces the disease progression (Zhang, et al. 2016). Cell based therapies include autologous chondrocyte implantation and bone marrow-derived mesenchymal stem cells. Tissue engineering includes cell-based scaffolds, cell-free scaffolds, and gene therapy.
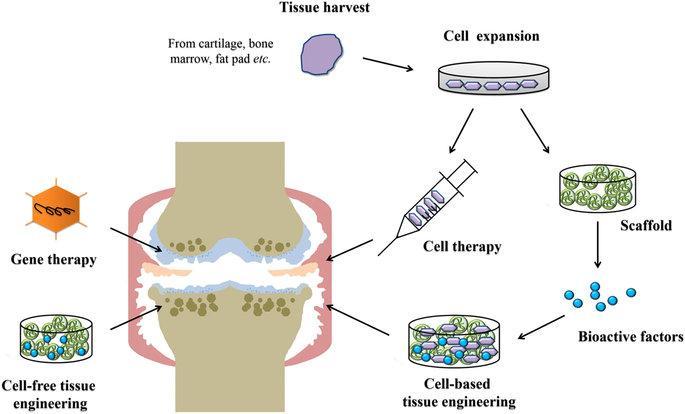
Figure 41: Current regenerative therapy for OA (Source: www.nature.com)
Surgical Procedures
Total hip and knee replacements offer excellent symptomatic relief and improved physical function. Surgical procedures are only recommended in those in whom the symptoms are refractory with non-pharmacological and pharmacological therapies. However, there are various factors on the decision of arthroplasty of hip or knee joints including patient’s willingness, time for the intervention, and complications of the procedure.

Figure 42: Knee replacement (Source: www.edition.cnn.com)
Prognosis
Marked disability is less in OA compared to RA. However, severe pain and functional impairment cause considerable limitations.
Economical Impact of the disease
OA of the knee joint is a major contributor to physical disability, especially among women. In 1990, osteoarthritis was the eighth leading cause of non-fatal burden disease, accounting for 2.8% of total years of living with disability globally. As the age advances, the risk of OA increases. So, as the life expectancy is increasing in developing countries, there is risk of increased number of osteoarthritis cases.
Disease Prevention
Weight reduction, non-risky exercise, maintenance of vitamin D and correction of length discrepancy reduces the symptoms of knee OA.
References
Allen, K.D., and Golightly, Y.M. (2015) Epidemiology of osteoarthritis: state of the evidence. Current Opinion in Rheumatology, 27(3), 276-283.
Anandacoomarasamy, A. (2010) Current Evidence for Osteoarthritis Treatments. Therapeutic Advances in Musculoskeletal Disease, 2(1), 17–28.
Bhatia, D., Bejarano, T., & Novo, M. (2013) Current interventions in the management of knee osteoarthritis. Journal of Pharmacy & Bioallied Sciences, 5(1), 30-38.
Boissonneault, A., Lynch, J.A., Wise, B.L., Seagal, N.A., Gross, K.D., Murray, D.W., et al. (2014) Association of hip and pelvic geometry with tibiofemoral osteoarthritis: Multicenter Osteoarthritis Study (MOST). Osteoarthritis Cartilage, 22(8), 1129–1135.
Brown, T.D., Johnston, R.C., Saltzman, C.L., Marsh, J.L., Buckwalter, J.A. (2006) Posttraumatic osteoarthritis: a first estimate of incidence, prevalence, and burden of disease. Journal of Orthopedic Trauma, 20(10), 739–744.
Chapman, K., Mustafa, Z., Dowling, B., Southam, L., Carr, A., Loughlin, J. (2002) Finer linkage mapping of primary hip osteoarthritis susceptibility on chromosome 11q in a cohort of affected female sibling pairs. Arthritis and Rheumatism, 46(7), 1780–1783.
Chen, T.H., Chen, L., Hsieh, M.S., Chang, C.P., Chou, D.T., and Tsai, S.H. (2006) Evidence for a protective role for adiponectin in osteoarthritis. Biochimica et Biophysica Acta, 1762, 711–718.
Cho, H.J., Chang, C.B., Kim, K.W., Park, J.H., Yoo, J.H., Koh, I.J., et al. (2011) Gender and prevalence of knee osteoarthritis types in elderly Koreans. The Journal of Arthroplasty, 26(7), 994-999.
Christensen, R., Astrup, A. and Bliddal, H. (2005) Weight loss: the treatment of choice for knee osteoarthritis? A randomized trial. Osteoarthritis and Cartilage, 13, 20–27.
Cirillo, D.J., Wallace, R.B., Wu, L., Yood, R.A. (2006) Effect of hormone therapy on risk of hip and knee joint replacement in the Women's Health Initiative. Arthritis and Rheumatism, 54(10), 3194–3204.
Cooper, C., Snow, S., McAlindon, T.E., Kellingray, S., Stuart, B., Coggon, D., Dieppe, P.A. (2000) Risk factors for the incidence and progression of radiographic knee osteoarthritis. Arthritis and Rheumatism, 43(5), 995–1000.
Felson, D.T., Zhang, Y., Hannan, M.T., Naimark, A., Weissman, B., Aliabadi, P., et al. (1997) Risk factors for incident radiographic knee osteoarthritis in the elderly: the Framingham Study. Arthritis and Rheumatism, 40(4), 728–733.
Gavura, S. (2011) Collagen: an implausible supplement for joint pain. Retrieved January 02, 2017, from https://sciencebasedmedicine.org/collagen-an-implausible-supplement-for-joint-pain/.
Grazio, S. & Balen, D. (2009) Obesity: risk factor and predictor of osteoarthritis. Lijeknicki Vjesnik, 131(1-2), 22-26.
Hardcastle, S.A., Dieppe, P., Gregson, C.L., Hunter, D., Thomas, G.E., Arden, N.K., et al. (2014) Prevalence of radiographic hip osteoarthritis is increased in high bone mass. Osteoarthritis Cartilage, 22, 1120–1128.
Harkey, M.S., Luc, B.A., Golightly, Y.M., Thomas, A.C., Driban, J.B., Hackney, A.C., et al. (2015) Osteoarthritis-related biomarkers following anterior cruciate ligament injury and reconstruction: a systematic review. Osteoarthritis Cartilage, 23, 1–12.
Hui, M., Doherty, M., and Zhang, W. (2011) Does smoking protect against osteoarthritis? Meta-analysis of observational studies. Annals of the Rheumatic Diseases, 70(7), 1231–1237.
Hunter Pain Clinic. (2016) Osteoarthritis. Retrieved January 03, 2017, from http://www.hunterpainclinic.com.au/index.cfm?module=NEWS&pagemode=indiv&page_id=580115.
Knutson, G.A. (2005) Anatomic and functional leg-length inequality: a review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: prevalence, magnitude, effects and clinical significance. Chiropractic Osteopathy, 13, 11.
Lee, K.M., Chung, C.Y., Sung, K.H., Lee, S.Y., Won, S.H., Kim, T.G., et al. (2015) Risk factors for osteoarthritis and contributing factors to current arthritic pain in south korean older adults. Yonsei Medical Journal, 56(1), 124-131.
Loughlin, J. (2001) Genetic epidemiology of primary osteoarthritis. Current opinion in rheumatology, 13(2), 111–116.
McDonough, C.M., & Jette, A.M. (2010) The contribution of osteoarthritis to functional limitations and disability. Clinics in Geriatric Medicine, 26(3), 387–399.
Messier, S.P., Loeser, R.F., Miller, G.D., Morgan, T.M., Rejeski, W.J., Sevick, M.A., et al. (2004) Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis and Rheumatism, 50, 1501–1510.
Murphy, L., Schwartz, T.A., and Helmick, C.G., Renner, J.B., Tudor, G., Koch, G.,et al. (2008) Lifetime risk of symptomatic knee osteoarthritis. Arthritis and Rheumatism, 59(9), 1207–1213.
Murray, K.J. & Azari, M.F. (2015) Leg length discrepancy and osteoarthritis in the knee, hip and lumbar spine. The Journal of the Canadian Chiropractic Association, 59(3): 226–237.
Neogi, T. (2013) The epidemiology and impact of pain in osteoarthritis. Osteoarthritis Cartilage, 21(9), 1145-1153.
Neogi, T., and Zhang, Y. (2013) Epidemiology of osteoarthritis. Rheumatic Diseases Clinics of North America, 39(1), 1–19.
Papadakis, M.A., McPhee, S.J., and Rabow, M.W. (2017) Current medical diagnosis & treatment. New York: McGraw Hill Education.
Sowers, M.R., and Karvonen-Gutierrez, C.A. (2010) The evolving role of obesity in knee osteoarthritis. Current Opinion in Rheumatology, 22(5), 533-537.
Toivanen, A.T., Heliovaara, M., Impivaara, O., Arokoski, J.P., Knekt, P., Lauren, H., et al. Obesity, physically demanding work and traumatic knee injury are major risk factors for knee osteoarthritis—a population-based study with a follow-up of 22 years. Rheumatology, 49(2), 308–314.
US Food and Drug Administration. (2011) FDA limits acetaminophen in prescription combination products; requires liver toxicity warnings. Silver Spring: FDA. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm239894.htm.
Valdes, A.M., and Spector, T.D. (2009) The genetic predisposition to osteoarthritis. IBMS BoneKEY, 6, 181-189.
Veronese, N., Stubbs, B., Noale, M., Solmi, M., Luchini, C., and Maggi, S. (2016) Adherence to the Mediterranean diet is associated with better quality of life: data from the Osteoarthritis Initiative. The American Journal of Clinical Nutrition, 104(5), 1403-1409.
Walker, B.R., Colledge, N.R., Ralston, S.H. & Penman, I.D. (2014). Davidson’s principles & practice of medicine. 2nd ed. New Delhi: Replika Press Pvt, pp. 1081-1086.
Wang Y, Simpson JA, Wluka AE, Teichtahl AJ, English DR, Giles GG, et al. (2011) Is physical activity a risk factor for primary knee or hip replacement due to osteoarthritis? A prospective cohort study. The Journal of rheumatology, 38(2), 350-357.
Yucesoy, B., Charles, L.E., Baker, B. & Burchfiel, C.M. (2015) Occupational and genetic risk factors for osteoarthritis: A review. Work, 50(2), 261-273.
Zhang, Y., and Jordan, J.M. (2010) Epidemiology of osteoarthritis. Clinics in Geriatric Medicine, 26(3), 355-369.
Zhang, W., Moskowitz, R.W., Nuki, G., Abramson, S., Altman, R.D., Arden, N., et al. (2008) OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis and Cartilage, 16, 137–162.
Zhang, W., Ouyang, H., Dass, C.R. and Xu, J. (2016) Current research on pharmacologic and regenerative therapies for osteoarthritis. Bone Research, 4, 15040.
Zhou, Q., Yang, W., Chen, J., and Wang, Y. (2012) Metabolic syndrome meets osteoarthritis. Nature Reviews Rheumatology, 8, 729-737.
Course Exam
Before you receive your certificate, you must complete the exam and achieve a score of % or higher. (You have unlimted attempts).
This exam is required by your state licensure.
Exam
Exam
We are required to delay the exam hours. Check back soon!
Exam
We are required to delay the exam until you have had time to view the course material. Please view the course first!
No Licenses on File
Please add a license to your account before you continue. Thank you!