Pediatric Abusive Head Trauma (Shaken Baby Syndrome)
Pediatric Abusive Head Trauma (Shaken Baby Syndrome)
Course Description
The focus of this course is pediatric abusive head trauma, and includes content regarding signs, symtoms, consequences, diagnosis and treatment.
Accreditation Information: KLA Education Services LLC is accredited by the State of California Board of Registered Nursing, Provider # CEP16145.
Course Certification: Once you have completed this course, click on the “Print Certificate” option below to save or print your CE course certification. If you are not yet registered in a course plan with IvyLeagueNurse, please complete the registration and payment process so that you are able to log into your account and fully obtain your course certificate. Our affordable and unlimited one-year CEU plan starts at just $19.99.
Print Certificate Print Course
Course Objectives
Upon completion of this course, the course participant will be able to:
- The definition of shaken baby syndrome
- History and incidence of child abusive head injuries
- Risk factors, clinical presentation and physical findings of shaken baby
- Mechanism of injury of shaken baby
- Diagnosis of abused child
- Outcome of shaken baby syndrome
- Management of head trauma in shaken babies
- Prevention of shaken baby syndrome
- Education about prevention of shaken baby syndrome
- Legal issues regarding child abusive head injuries
Course Content
Course Description
This course briefly describes about shaken baby syndrome (head injuries to babies due to abuse), regarding its definition, incidence, risk factors, mechanism of head injuries, clinical manifestations, diagnosis management, prognosis, prevention and legal issues. This course provides nurses and other professionals with comprehensive approach to recognize and manage a baby of abusive head injuries. Valuable tools are described in this course regarding prevention of shaken baby syndrome. A healthy description is also given about legal issues regarding abusive head injuries of babies/children.
Definition
‘Shaken Baby Syndrome’ is a term which is used to define severe types of head injuries in infants and children, inflicted on them during the course of abuse. Medically, it is characterized by three consequences of head injury i.e.
-
Subdural Hematoma
-
Retinal hemorrhages
-
Cerebral edema
Such injuries result from intentional shaking of child during abuse and in most of such cases there is no significant sign of external injury. Even 5 seconds of intentional shaking can cause such type of head injuries.
Shaken baby syndrome is common among children younger than 2 years of age but may be present in children up to age of five. Besides intentional shaking, abusive head trauma in children can be caused by direct blows to the head and dropping or throwing a child. The consequences of shaking babies or toddlers may include (1):
-
Complete recovery
-
Brain damage
-
Blindness
-
Deafness
-
Speech and learning problems, including mental retardation
-
Fits
-
Neck and spinal cord injury, which can cause to motor abnormality ranging in severity from mild weakness to paralysis
Other names used for Shaken Baby Syndrome are:
-
Whiplash shaken infant syndrome
-
Abusive head trauma
-
Shaken impact syndrome
-
Inflicted head injury (1,2)
Evolution of “Shaken Baby Syndrome”
John Caffey was a pediatric radiologist. In 1946, he told the relationship of long bone fractures of abused children with head injuries. He advised physicians and surgeons to look for intracranial injuries in children presented with fractures of bones and vice versa. Norman Guthkelch first time described the shaking as a mechanism/cause of intracranial injuries of the abused child in 1971. He also demonstrated the association of retinal hemorrhages with shaking. In 1972, Caffey introduced a term ‘Whiplash shaken infant syndrome.’ According to Caffey this syndrome was characterized by (1):
-
Intracranial injuries
-
Long bone fractures
-
Retinal hemorrhages
It was the 1980s when the term Shaken baby syndrome was used to describe these three findings. Shaken impact syndrome was another term introduced to describe the above three findings along with features of impact injuries to brain, skull and soft tissues in an abused child. The term abusive head trauma was introduced by Kent Hymel in 1990 to describe these findings. Recently, the American Academy of Pediatrics Committee on Child Abuse and Neglect advised to use the term “abusive head trauma” in cases of intentional shaking of babies as it is a good description for such inflicted injuries, but the shaken baby syndrome is still widely used term (3-5).
Incidence, Mortality and Morbidity
In US, the leading cause of death in child abuse issues is shaken baby syndrome or abusive head trauma. Regarding incidence, mortality and morbidity in cases of shaken baby syndrome, following facts are important (1,6):
-
No reliable statistic is available on prevalence of shaken baby syndrome in US.
-
Mortality rate of shaken baby syndrome ranges from 15-25% (median is 20-25%) and almost 50% of deaths are reported due to shaken baby syndrome.
-
Almost 1200 to 1400 cases/year of this syndrome are reported in the US. One in 4 of these babies die, and only about one-third will survive without severe dysfunction.
-
2 million children are abused each year in the US alone.
-
In 6% of the reported cases of child abuse, an eye specialist is responsible for initial identification of the abuse.
-
The age of the victim of this syndrome ranges from just a few days to five years, with an average of 6-8 months.
-
Men are the usual culprit for this syndrome, in almost 80% cases (especially young adults of age in early 20s).
-
Females who shake children or babies tend to be caregivers.
-
As child abuse is a hidden event, so many cases of this syndrome are not reported or presented in some other forms such as fall or an accident.
-
Boys are shaken more than girls (1,6).
Mechanism of Injury in Shaken Baby Syndrome
It is very important to remember that shaken injuries are usually not caused by falls or impact from normal plays which cause linear forces (4). It is the rotational force that causes shaken head injuries. So, shaken head injuries occur when someone shakes a baby. Anatomical differences of infants put them on high risk of getting head injuries during shaking and therefore, the majority of victims are babies of less than one year of age. Forceful shaking of child causes child’s head to rotate about neck uncontrollably, as child’s neck muscles are not mature enough to support the head properly. This potential movement pitches the baby’s brain back and forth within the skull, sometimes causing rupture of blood vessels and nerves throughout the brain and ultimately tears the brain tissue. The brain tissue may hit the inner surface of the skull, causing bruising and bleeding to the brain matter. The injury can be even more lethal when a shaking interval ends with an impact (such as hitting a wall or a crib mattress), as the forces of acceleration and deceleration associated with such impact are so powerful (7,8). Shaking can cause swelling in the brain and leads to very high pressure within the skull, compressing blood vessels and enhancing the overall injury to its soft structure. Though these injuries are reported in children up to five years of age but the average age for this syndrome ranges between 3-8 months. Most often parents or caregivers are the culprits of these injuries (9).
Causes and Risk Factors
Factors that Put an Infant at Risk
There are many factors that can enhance an infant’s risk of being shaken especially when combined with a parent or a caregiver who is not ready to cope with caring for a baby. These include:
-
Children with age of less than 1 year
-
Though babies of less than 1 year of age are at the greatest risk, but this syndrome has also been reported in children up to 5 years of age.
-
Babies with age of 2-4 months are especially at risk of getting injury from shaking, as they are small in relation to the size of adults who may pick them up and shake them, and they cry more frequently and longer than older babies.
-
Premature infants
-
Disable infants
-
Being one of a multiple birth
-
Inconsolable and/or frequent crying
-
Prior physical abuse or prior shaking (2,5)
-
Most victims are male.
Factors that Can Enhance Parents’ or Caregivers’ Risk for Shaking a Baby
Parents and their partners are the main culprits with the majority of the perpetrators being the male parent or partner. There are numerous factors which increase a parent’s or caregiver’s risk of shaking a baby, especially when combined with not being prepared to cope with caring for a baby. These include:
-
Anger due to an infant’s crying
-
Being tired
-
Having limited anger management
-
No or limited social support
-
Young age of parents
-
Unstable family situation
-
Low socioeconomic status
-
Unrealistic expectations about child development and child-rearing
-
Rigid attitudes
-
Impulsivity
-
Feelings of inadequacy, isolation, or depression
-
Being a victim or witness to intimate partner violence
-
Negative childhood experiences, including neglect or abuse (10)
Signs and Symptoms
Following types of injuries can occur in shaken babies:
-
Subdural hematoma
-
Retinal hemorrhages
-
Long bone fractures
-
Increased intracranial pressure
-
Hydrocephalus
-
Soft tissues injuries that cannot be explained by accidental trauma or some medical disease
-
Diffuse axonal injury
-
Cerebral edema (7,11,12)
Signs and symptoms depend upon duration and severity of injury. Following are signs and symptoms of shaken baby syndrome (13,14):
-
Lethargy
-
Irritable behavior
-
Vomiting and nausea
-
Poor sucking or swallowing ability
-
Decreased appetite
-
No smiling or vocalizing
-
Spasticity
-
Fits
-
Shortness of breath
-
Altered level of consciousness
-
Unequal pupil size
-
An inability to lift the head
-
An inability to focus the eyes
-
Pale and bluish skin
-
Vision loss
-
Physical signs like bruising, swelling or bleeding may be absent
-
Forehead bulging
-
Tremors (15)
Consequences of Shaking
Shaking often leads to irreversible damage. In the more severe cases, babies die due to severe injuries. Babies who survive may have one or more of the following long term defects (16,17):
-
Blindness
-
Deafness
-
Convulsions or epilepsy
-
Delayed developmental milestones
-
Impaired intellect
-
Speech and learning defects
-
Memory and attention deficits
-
Severe mental retardation
-
Cerebral palsy
In mild cases children look normal just after shaking but they may eventually develop one or more of above described defects. In some cases, child may remain asymptomatic until he or she enters the education system and exhibits learning difficulties and behavioral problems (18).
Diagnosis
Nurses or other health care providers may suspect shaken baby syndrome whenever they find any of the following:
-
Any child who presents with a history that is not consistent with the presenting complaints and physical findings
-
The presence of a new partner in the home
-
History of delay in seeking medical attention
-
Previous history or suspicion of abuse
-
The absence of a primary caregiver at the onset of injury or illness
-
Physical evidence of multiple injuries at varying stages of healing
-
Unexplained changes in neurologic examination
-
Unexplained shock
-
unexplained cardiovascular shut down (17)
Following tools may be used for diagnosing a case of shaken baby syndrome:
-
X-rays skull for skull fractures
-
Eye emanation by an experienced ophthalmologist to check for retinal hemorrhages
-
MRI can also detect retinal hemorrhages
-
CT-scan head and MRI to detect intracranial injuries (18)
Treatment
Treatment of shaken baby syndrome depends upon the type of intracranial injuries. Following steps may be carried to treat a shaken baby:
-
Call your local emergency number as immediate emergency treatment may be needed.
-
You can start CPR if the child stops breathing till the emergency help arrives.
-
Vomiting may be the presenting symptom in shaken baby along with altered level of consciousness and there may be chances of aspiration in such babies. If there is no spinal injury then turn the baby’s head to one side to prevent aspiration or choking. If there is spinal injury, turn the whole baby’s body carefully to one side.
-
Do not shake the baby to wake him or her up.
-
Do not give the child anything by mouth.
-
Monitor intracranial pressure.
-
Decrease the raised intracranial pressure by drugs (mannitol) or by surgical drainage of brain ventricles.
-
Drainage of subdural hematoma if possible.
-
Management of bone fractures if present.
-
Management of soft tissues injuries if present (1).
Prevention
Socio-ecological Model
Prevention demands the understanding of the factors that affect violence. The CDC utilizes four level socio-ecological model to understand the concept of violence and the influence of preventive measures. Socio-ecological model uses the complex interplay between individual, relationship, community and social factors. You can use this model as practical framework to make your strategy.
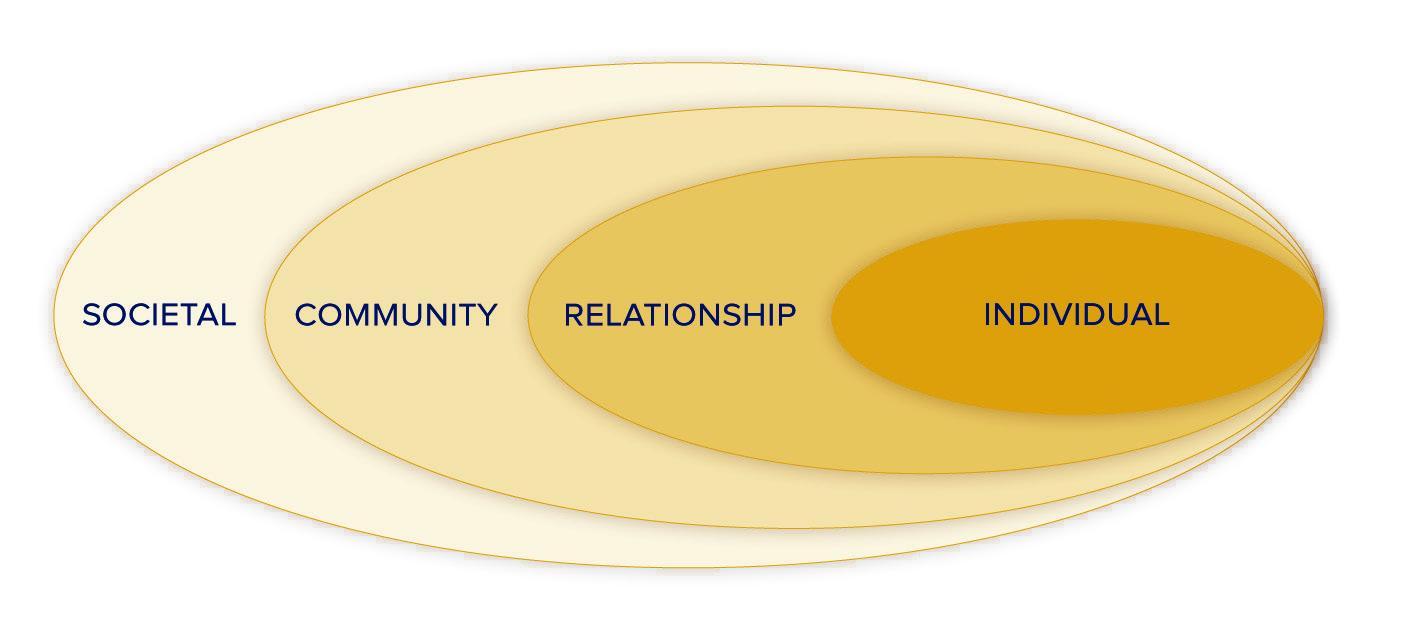
-
Individual-level strategies are aimed at changing the knowledge and skills of parents or caregivers.
-
Relationship-level strategies are aimed at changing the interactions between
-
People—parents and children
-
Parents and other caregivers
-
Parents and health care providers, bystanders, and parents
-
Community-level strategies are aimed at changing the properties of settings that give rise to violence or that protect against violence e.g.
-
Address social and economic factors.
-
Access and availability of parental support programs.
-
Early child care
-
Respite care centers
- Societal-level strategies are used to change cultural norms surrounding parenting, as well as laws and policies aimed at supporting parents.
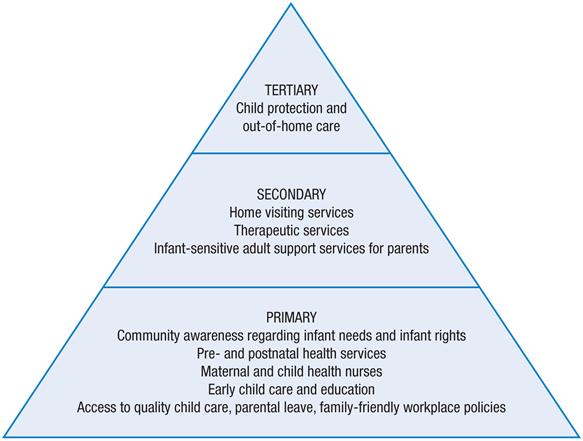
Learning From Existing Programs
You must begin with what is available, feasible and has the highest level of effectiveness. There are many shaken baby syndrome prevention programs available which can be used. Many of these programs are trying to:
-
raise the awareness about abusive head trauma
-
educate parents and caregivers about the consequences of shaking a baby
-
tell parents and caregivers about baby crying behavior
-
explain parents and caregivers safe ways to reduce and prevent shaking baby syndrome injuries
Examples of Prevention Strategies:
- Coordinated hospital-based primary prevention programs tackle the parents of newborns
-
Home visits for new parents- Here health professionals give:
-
Information
-
Health care
-
Psychological support
-
Other services that can help community to be more efficient parents and caregivers
-
-
Anticipatory guidance at well-baby visits in pediatric practice and/or health clinics
-
School prevention programs for junior high and high school students- These programs provide students with consideration of:
-
Child maltreatment cases
-
Anger management measures
-
And child care methods
-
-
Programs targeting males, especially new fathers
-
Professional education and trainings for doctors, nurses, social workers
-
Educational print and video materials
“The Period of Purple Crying” and it’s Role in Prevention
Shaking baby syndrome is 100% preventable issue. Period of PURPLE Crying is a preventive program provided by The National Center on Shaken Baby Syndrome. This program helps the parents and other caregivers understand crying in normal babies. Being a health care providers you must make parents and caregivers familiar with this program, by doing so, you can help prevent child abusive trauma. The following table describes the points of this preventive program (19,20):
Table 1= source: national Center on shaken baby syndrome
| P - Peak Pattern | Crying peaks around 2 months, then decreases. |
| U - Unpredictable | Crying for long periods can come and go for no reason. |
| R - Resistant to soothing | Crying for long periods can come and go for no reason. |
| P - Pain | Baby has a pain-like look on the face. |
| L - Long bouts of crying | Crying can go on for hours. |
| E - Evening crying | Crying occurs mostly in afternoon and evening. |
Dr. Harvey Karp's "Five S" Method may provide guidance in helping to sooth a crying baby.
-
Shushing (using "white noise" or rhythmic sounds that mimic the constant whir of noise in the womb, with things like vacuum cleaners, hair dryers, clothes dryers, a running tub, or a white noise CD)
-
Side/stomach positioning (placing the baby on the left side — to help digestion — or on the belly while holding him or her, then putting the sleeping baby in the crib or bassinet on his or her back)
-
Sucking (letting the baby breastfeed or bottle-feed, or giving the baby a pacifier or finger to suck on)
-
Swaddling (wrapping the baby up snugly in a blanket to help him or her feel more secure)
- Swinging gently (rocking in a chair, using an infant swing, or taking a car ride to help duplicate the constant motion the baby felt in the womb)
Other Techniques to Cope with Crying Infants
You may also try the following steps to cope with a crying infant: (source: www.kidshealth.org)
-
Be sure that the baby’s basic needs are met.
-
Examine for signs of illness.
-
Walk with the baby.
-
Sing / talk to the baby.
-
Give the baby a noisy toy.
-
Take the baby for a ride in a stroller.
-
Bring the baby close against your body and breathe calmly and slowly.
-
Call a friend for help or to take care of the baby while you take a break.
-
If you are still failing then keep the baby on his or her back in the crib, close the door, and check on the baby in 10 minutes.
-
Call your doctor if nothing seems to be helping your infant (7,19).
References
-
Shaken Baby Syndrome [Internet]. [Last updated 2013 Oct 17; cited on 2013 Oct25]. Available from: http://en.wikipedia.org/wiki/Shaken_baby_syndrome.
-
Herman BE, Makoroff K L, Cornelli HM. Abusive head trauma. Pediatr Emerg Care 2011;5(1):65-9.
-
Walls C. Shaken baby syndrome education: a role for nurse practitioners working with families of small children. J Pediatr Health Care 2006;20 (5):304-10.
-
Hymel KP, Deye KP. Abusive head trauma. In: Jenny C. Child Abuse and Neglect.St. Louis, MO: Saunders; 2011:349-358.
-
Ceballos SG. Abusive head trauma: a case study. Adv Emerg Nurs J 2009;31(4):277.
-
Shaken Baby Syndrome [Internet]. [Last updated 2011 Jan 24; cited on 2013 Oct 25]. Available from: http://www.nlm.nih.gov/medlineplus/ency/article/000004.htm.
-
Foeller EC. Shaken Baby Syndrome [Internet]. [Last updated 2011 Jan; cited on 2013 Oct25]. Available from: http://kidshealth.org/parent/medical/brain/shaken.html#.
-
Oral R, Yagmur F, Nashelsky M, Turkman M, Kirby P. Fatal abusive head trauma cases.Pediatr Emerg Care 2008;24(12):816-21.
-
Mraz MA. The physical manifestations of shaken baby syndrome. J Forensic Nurs 2009;5:26-30.
-
Miehl N J. Shaken baby syndrome. J Forensic Nurs 2005;1(3):111-17.
-
What is shaken baby syndrome? [Internet]. [Last updated 2012 March4; cited on 2013 Oct 25]. Available from: http://www.babycenter.com/0_shaken-baby-syndrome_1501729.bc.
-
Waseem M, Pinker H. Apparent life-threatening event or child abuse? Pediatr Emerg Care 2006;22(4):245-6.
-
Tung GA. Imaging of abusive head trauma. In: Jenny C. Child Abuse and Neglect. St. Louis, MO: Saunders; 2011:373-91.
-
Levin AV. Eye injuries in child abuse. In: Jenny C. Child Abuse and Neglect. St. Louis, MO: Saunders; 2011:402-412.
-
Kriss VM. Imaging of skeletal trauma in abused children. In: Jenny C. Child Abuse and Neglect. St. Louis, MO: Saunders; 2011:296-307.
-
Shaken Baby Syndrome [Internet]. [Last updated 2011; cited on 2013 Oct25]. Available from: http://my.clevelandclinic.org/childrens-hospital/health-info/diseases-conditions/neurological-conditions/hic-Shaken-Baby-Syndrome.aspx.
-
Chiesa A, Duhaime A. Abusive head trauma. Pediatr Clin North Am 2009;56:317-31.
-
Matschke J, Herrmann B, Sperhake J, Korger F, Bajanowski T, Glatzel M. Shaken baby syndrome. Deutsches Arzteblatt Intl 2008;106(13):211-7.
-
Dias MS, Smith K, deGuehery K, Mazur P, Li V, Shaffer ML. Preventing abusive head trauma among infants and young children: a hospital-based, parent education program. Pediatrics 2005;115(4):470-7.
-
Smith KM, deGuehery KA. Shaken baby syndrome education program: nurses making a difference. MCN 2008;371-5.
Course Description
Course Objectives
Course Content
- Course Description
- Evolution of “Shaken Baby Syndrome”
- Incidence, Mortality and Morbidity
- Mechanism of Injury in Shaken Baby Syndrome
- Causes and Risk Factors
- Signs and Symptoms
- Consequences of Shaking
- Diagnosis
- Treatment
- Prevention
- Learning From Existing Programs
- “The Period of Purple Crying” and it’s Role in Prevention
- Other Techniques to Cope with Crying Infants
- References
Course Exam
Before you receive your certificate, you must complete the exam and achieve a score of % or higher. (You have unlimted attempts).
This exam is required by your state licensure.
Exam
Exam
We are required to delay the exam hours. Check back soon!
Exam
We are required to delay the exam until you have had time to view the course material. Please view the course first!
No Licenses on File
Please add a license to your account before you continue. Thank you!