Alzheimer's Disease
Alzheimer's Disease
Course Description
This course covers aspects of caregiving for Alzheimer's Disease patients, including disease stages and risk factors about which nursing professionals should be aware.
Accreditation Information: KLA Education Services LLC is accredited by the State of California Board of Registered Nursing, Provider # CEP16145.
Course Certification: Once you have completed this course, click on the “Print Certificate” option below to save or print your CE course certification. If you are not yet registered in a course plan with IvyLeagueNurse, please complete the registration and payment process so that you are able to log into your account and fully obtain your course certificate. Our affordable and unlimited one-year CEU plan starts at just $19.99.
Print Certificate Print Course
Course Objectives
Upon completion of this course, the course participant will be able to:
- to be familiar with the history of Alzheimer’s disease.
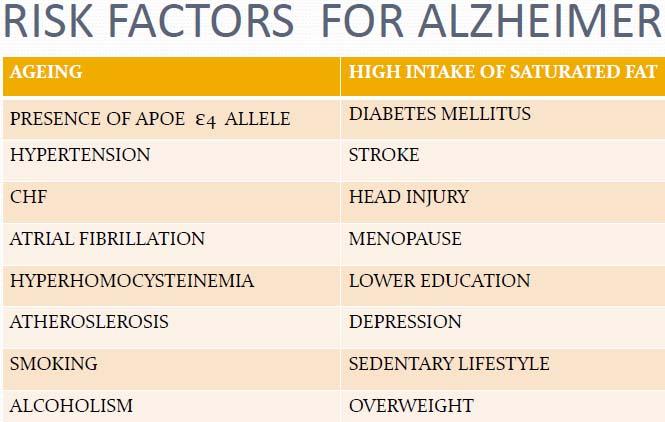
- to list 5 risk factors for Alzheimer’s disease.
- to list 10 components of care giving for Alzheimer’s disease.
- to describe the 7 stages of Alzheimer’s disease.
- to be familiar with nursing role strain for care givers to those with Alzheimer’s disease.
- to be familiar with nursing interventions for patients and families.
Course Content
Alzheimer’s Disease
Progressive mental deterioration in old age has been recognized and described throughout history. However, in was not until the early part of the 20th century that a collection of brain cell abnormalities were specifically identified by Dr. Alois Alzheimer, a German physician, in 1906 (A History, 2006). He lectured about a woman who had died after years of experiencing severe memory problems, confusion, and difficulty understanding questions. Upon her death, he performed an autopsy on her brain and described dense deposits outside and around the nerve cells (neuritic plaques). Inside the nerve cells he noted the presence of twisted bands of fibers (neurofibrillary tangles). Today, this degenerative brain disorder bears his name. The observation of the plaques and tangles at autopsy is still required to obtain a definitive diagnosis of Alzheimer's disease (A History).
The majority of Alzheimer’s disease cases are late-onset, usually developing after age 65 (A History, 2006). Late-onset Alzheimer’s disease has no known cause and shows no obvious inheritance pattern. However, in some families, clusters of cases exist. Genetic risk factors alone are not enough to cause the late-onset form of Alzheimer’s disease, so researchers are actively exploring education, diet, and environment to learn what role they might play in the development of this disease (A History).
Although the diagnosis of Alzheimer's can still only be made through an autopsy, clinicians can now make an accurate diagnosis 90% of the time by taking a history, performing a physical examination, utilizing medical tests, ruling out other causes, and measuring memory capabilities and psychological status. Early diagnosis is important because the treatments that are available work best at the earliest stages of the disease (A History, 2006). There is no known treatment that will cure Alzheimer's disease. For those who are currently suffering with the disease, medications can only help control symptoms and/or slow the progression of the disease (A History). It is only one of several forms of dementia. A diagnosis of Alzheimer's disease for a living family member means a definitive diagnosis for other causes of dementia have been ruled out. Other causes may be stress, depression, nutrition deficiencies, stroke, Parkinson's disease, drug side effects, or even AIDS (Alzheimer's Facilities, 2006).
Alzheimer’s disease is not only a devastating experience for those that suffer from it, but also a major life burden for the caregivers. The role caregivers fill is a very stressful undertaking that may last for many years. Nurses may have the best opportunity of anyone to make a difference in the life of an Alzheimer’s disease caregiver.
Review of Literature
Literature exists in all aspects of the disease. Depression has been the most frequently studied mental health symptom for Alzheimer’s disease caregivers (Schulz, O’Brien, Bookwala, & Fleissner, 1995). Evidence strongly supports that Alzheimer’s disease caregivers are more depressed than sociodemographically comparable individuals who are not caregivers (Coope et al., 1995). Primary caregivers were defined as unpaid persons who had the primary responsibility of helping a patient with activities of daily living and instrumental activities of daily living (Kuzu et al, 2005). Overall mental health scores and the subscales of anxiety, depression, positive affect, and feelings of belonging were significantly poorer for wife caregivers. The wide variances for mental health scores among caregivers reflected that some of caregivers were having a great deal more difficulty coping with the challenging conditions in their lives than other caregivers (Willette-Murphy, Todero, & Yeaworth, 2006). Research has found that caring for a family member with Alzheimer’s disease is a highly stressful experience (Beeson, Horton-Deutsch, Farran, & Neundorfer, 2000). Adverse effects on the mental health of Alzheimer’s disease caregivers, especially in the form of depression, have been reported to be much higher than either age or gender-based population norms or noncaregiving control groups (Beeson et al). The emotional strain of witnessing and adapting to a family member’s cognitive, behavioral, and personality changes often contribute to depressive symptoms (Beeson et al).
Care Giving Responsibilities
Pre-placement
-
Frequent visits
-
Monitoring of loved one (e.g., eating,bathing, grooming, toileting, taking medications, safety issues such as wandering)
-
Meal preparation
-
Laundry and clothing maintenance
-
Cognitive assistance (e.g., orienting)
-
Money management (e.g., check writing)
-
Medical appointments and consults
-
Cleaning and grounds upkeep
-
Moving parent to smaller home or apartment
-
Day care
Post-placement
-
Frequent visits
-
Monitoring of care (e.g., eating, bathing, grooming, skin-care, toileting, medications)
-
Feeding assistance
-
Laundry and clothing maintenance
-
Mental stimulation through visits and encouragement of loved one’s participation in activities at nursing home
-
Money management (e.g., paying bills and maintaining social security, Medicaid, personal needs accounts)
-
Medical appointments, consults, resident careplanning meetings
Source: Garity, J. (2006)
Loneliness as a factor in the development of depression in the Alzheimer’s disease caregiver has been given little attention, despite the fact that researchers have found moderate to high correlations between loneliness and depression for many years (Beeson et al, 2000). How family caregivers cope with the burden of post nursing home placement of a family member with Alzheimer’s disease has also been researched. Several factors that positively or negatively affected coping among family caregivers were identified. Family caregivers’ interactions with their loved one, other nursing home residents, family and friends, nursing staff, and nursing home-sponsored support groups all contributed positively to their coping with the burden of post-nursing home placement (Beeson et al).
Impact on Gerontologic Nursing
The nurse should be aware of the progression of the disease process including overall symptoms and specific stage characteristics. This will allow for accurate and timely education and empowerment to the clients and caregivers of clients. Alzheimer’s disease has many progressive manifestations including loss in short term memory, wandering, episodes of agitation, depression, disorientation and confusion, incontinence, loss of weight, sleeplessness, and forgetfulness regarding functions of daily living (Alzheimer's Facilities, 2006).
There are seven stages to the disease progression. Stage one is no cognitive decline. It is described as no subjective complaints of memory deficit and no memory deficit evident on clinical interviews (The Stages, 2006). Stage two is very mild cognitive decline. The most frequent subjective complaints of memory deficit are forgetting where one has placed familiar objects and forgetting names one formerly knew well. There is no objective evidence of memory deficit on clinical interview and no objective deficits in employment or soial situaions, (The Stages).
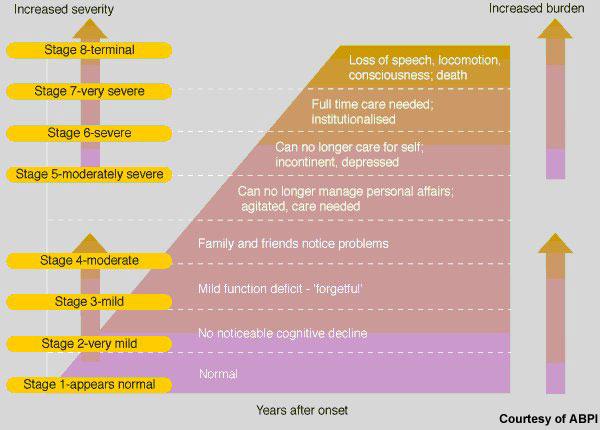
Stage three is early confusion, mild cognitive decline with earliest clear-cut deficits. Manifestations are in more than one of the following areas: patient may have gotten lost when traveling to an unfamiliar location; co-workers become aware of patient's relatively low performance; word and name finding deficit becomes evident to intimates; patient may read a passage of a book and retain relatively little material; patient may demonstrate decreased facility in remembering names upon introduction to new people; patient may have lost or misplaced an object of value; or concentration deficit may be evident on clinical testing. Objective evidence of memory deficit obtained only with an intensive interview. Denial begins to become manifested in patient. Mild to moderate anxiety accompanies symptoms (The Stages, 2006).
Stage four, late confusional moderate cognitive decline, is a clear-cut deficit on careful clinical interview (The Stages, 2006). Stage four deficit manifest in following areas: decreased knowledge of current and recent events; may exhibit some deficit in memory of one's personal history; concentration deficit elicited on serial subtractions; and decreased ability to travel, or handle finances. There are frequently no deficits in the following areas: orientation to time and person; recognition of familiar persons and faces; or ability to travel to familiar locations. The inability to perform complex tasks and denial are dominant defense mechanism. Flattening of affect and withdrawal from challenging situations occurs (The Stages).
Stage five, early dementia with moderately severe cognitive decline, requires assistance for the patient to survive (The Stages, 2006). During interview the patient is unable to recall a major relevant aspect of their current lives, e.g., an address or telephone number of many years, the names of close family members, the name of the high school or college from which they graduated (The Stages). There is frequently some disorientation to time or to place. An educated person may have difficulty counting back from 40 by fours or from 20 by twos. Persons at this stage retain knowledge of many major facts regarding themselves and others (The Stages). They invariably know their own names and generally know their spouse's and children's names. They require no assistance with toileting and eating, but may have some difficulty choosing the proper clothing to wear (The Stages).
Stage six involves middle dementia with severe cognitive decline (The Stages, 2006). The patient may occasionally forget the name of the spouse upon whom they are entirely dependent for survival and will be largely unaware of all recent events and experiences in their lives. They also retain some knowledge of their past lives but this is very sketchy. Generally, they are unaware of their surroundings, the year, or the season (The Stages, 2006). They may have difficulty counting from 10, both backward and sometimes forward. They will require some assistance with activities of daily living, may become incontinent, and will require travel assistance but occasionally will display ability to familiar locations. Almost always they recall their own name and frequently continue to be able to distinguish familiar from unfamiliar persons in their environment (The Stages).
Personality and emotional changes occur. These are quite variable and include: delusional behavior such as patients may accuse their spouse of being an impostor; they may talk to imaginary figures in the environment or to their own reflection in the mirror; obsessive symptoms, such as the person may continually repeat simple cleaning activities; anxiety agitation and even previously nonexistent violent behavior may occur; and loss of willpower because an individual cannot carry a thought long enough to determine a purposeful course of action (The Stages, 2006).

Stage seven, late dementia, is very severe cognitive decline. All verbal abilities are lost. Frequently there is no speech at all, incontinence of urine, and requires assistance toileting and feeding. They often lose basic psychomotor skills, the ability to walk, and sitting and head control. The brain appears to no longer to be able to tell the body what to do. Generalized and cortical neurologic signs and symptoms are frequently present (The Stages, 2006).
Solutions for Change
In order for loneliness and depression to be addressed, nurses’ knowledge, assessment, and diagnosis of loneliness in Alzheimer’s disease caregivers must be improved. Nursing interventions that alleviate controllable factors leading to loneliness and ultimately depression must be developed and implemented. Loneliness is not an irreversible condition of life, it is a treatable one. Although certain conditions of the Alzheimer’s disease caregiver’s life are not amenable to change, clinicians need to focus on those that are and develop practical interventions (Beeson et al, 2000). Because the eventual loss of ability to interact or carry on a normal conversation is a distinguishing characteristic of individuals with Alzheimer’s disease, nurses must better prepare family members to cope with this situation (Garity, 2006).
Diagnosing and implementing some of the following will ease caregiver role strain. For impaired social interaction, give info to the family about the support mechanisms, tell the patients and the caregivers to be open in their feelings, and tell the family to identify the possible persons who could give social support (Kuzu et al, 2005). Caregiver role strain determines the areas of difficulty being experienced with giving care. The nurse should assist the caregiver to express their feelings about the patient and their care, and make suggestions about sharing roles with family members. To aid with ineffective individual coping the nurse should develop constructive and trusting communication with the patient, ensure that the problems being experienced are recognized and prioritized, and be encouraging to the idea that they will be able to find a way to cope with their problems (Kuzu et al).
Ineffective family coping should involve discussing ineffective methods of individual coping that are used, and helping them to list their family problems. Altered family processes should be handled by meeting together with family and sharing their problems with other families experiencing the same problems, researching what support groups and organizations are available that can help with the patient’s home care and housework, receiving support from other individuals for help, sharing their feelings and thoughts about their new role and responsibilities as family individuals, and supporting each other in being able to cope. (Kuzu et al, 2005)
Conclusion and Reflection
Alzheimer's disease is a progressive, irreversible brain disorder with no known cause or cure. It attacks and slowly steals the minds of its victims. Always fatal, Alzheimer's disease is the most common form of irreversible dementia (About Alzheimer’s, 2006). More than 5.4 million Americans are believed to have Alzheimer’s disease and by 2050, the number could increase to 13.2 million. Approximately 82,000 victims die and 350,000 new cases of Alzheimer's disease are diagnosed each year (About Alzheimer’s). In every nation where life expectancy has increased, so has the incidence of Alzheimer's disease. Alzheimer's disease is becoming tragically common. It is estimated that there are currently 18 million people worldwide with Alzheimer’s disease. This figure is projected to nearly double by 2025 to 34 million people (About Alzheimer’s).

Alzheimer's disease research, a program of the American Health Assistance Foundation, was established in 1985 to fund research on and educate the public about Alzheimer's disease (About Alzheimer’s, 2006). Given a review of the history, there seems to be no cure in our near future. This is even more reason for nurses to be prepared to care for clients with Alzheimer’s disease and their caregivers.
Every healthy, happy human being is a dependent personality, searching for a bond of intimacy, a sense of belonging with and to another human being. Human beings need another self with which to share feelings, values, and decisions, mirroring through another and bringing recognition and awareness to their existence in the universe (Kuzu et al, 2005). The husband-wife and child-parent relationships were built on these human needs. In the Alzheimer’s disease caregiving process, one of the partners has emotionally and psychologically withdrawn. Losing the element of reciprocity in the relationship fosters feelings of loneliness and depression (Kuzu et al).
With loneliness comes an unwelcome feeling of lack or loss of companionship, an unpleasant aspect of missing certain relationships as well as missing a certain level of quality in one’s relationship (Kuzu et al, 2005). Nurses need to be active and take the leading role in research and self-education of Alzheimer’s disease. Being aware of the progression and stages of Alzheimer’s disease allows the nurse to be proactive in screening patients for early signs of the disease. Knowing useful interventions will help the nurse to empower the client and client’s caregivers to improve the life that lay ahead of them. It is important for nurses to maintain a rapport with clients that will allow free flow of information from the client’s caregiver. Caregivers should be continually assessed for stressors, with effective techniques for caregiving, methods of appraising their own health needs, and healthful living strategies. The prepared nurse can continually help solve these problems through assessment, diagnosis, planning, implementation, and evaluation.
References
A history of alzheimer's disease. (2006). Retrieved September 01, 2013, from American Health Assistance Foundation Web site: http://www.ahaf.org/alzdis/about/adhistory.htm
About alzheimer's disease. (2006). Retrieved September 01, 2013, from American Health Assistance Foundation Web site: http://www.ahaf.org/alzdis/about/adabout.htm
Alzheimer's facilities. (2006). Retrieved September 01, 2013, from Senior Resource Web site: http://www.seniorresource.com/haf.htm
Beeson, R., Horton-Deutsch, S., Farran, C., & Neundorfer, M. (2000). Loneliness and depression in caregivers of persons with alzheimer's disease or related disorders [Electronic version]. Issues in Mental Health Nursing, 21, 779-806.
Coope, B., Ballard, C., Saad, K., Patel, A., Bentham, P., Bannister, C., & et al. (1995). The prevalence of depression in the careers of dementia sufferers disorders [Electronic version]. International Journal of Geriatric Psychiatry, 10, 237–242.
Garity, J. (2006). Caring for a family member with alzheimer's disease disorders [Electronic version]. Journal of Gerontological Nursing. 39-48.
Kuzu, N., Beser, N., Zencir, M., Sahiner, T., Nesrin, E., Ahmet, E., & et al. (2005). Effects of a comprehensive educational program on quality of life and emotional issues of dementia patient caregivers disorders [Electronic version]. Geriatric Nursing, 26, 378-385.
Schulz, R., O’Brien, A., Bookwala, J., & Fleissner, K. (1995). Psychiatric and physical morbidity effects of dementia caregiving: Prevalence, correlates, and causes disorders [Electronic version]. The Gerontologist, 35, 771–791.
The stages of alzheimer's disease. (2006). Retrieved September 01, 2013, from EC-Online Web site:
http://www.ec-online.net/Knowledge/Articles/alzstages.html
Course Exam
Before you receive your certificate, you must complete the exam and achieve a score of % or higher. (You have unlimted attempts).
This exam is required by your state licensure.
Exam
Exam
We are required to delay the exam hours. Check back soon!
Exam
We are required to delay the exam until you have had time to view the course material. Please view the course first!
No Licenses on File
Please add a license to your account before you continue. Thank you!